ORIGINAL ARTICLES
Noise levels in a pediatric intensive care unit: an observational and correlational study
Fernanda Maria do Carmo da Silveira Neves de Oliveira1, Márcia Barbosa de Paiva1, Maria Aparecida de Luca Nascimento1, Vivian Marinho Rezende1, Alexandre Sousa da Silva1, Carlos Roberto Lyra da Silva1
1Federal University of the State of Rio de Janeiro
ABSTRACT
Aim: To measure noise levels in a pediatric intensive care customer unit and discuss the consequences of such noise in relation to professional actions.
Method: This is an observational and correlational study, performed in the pediatric intensive care unit of a federal hospital in Rio de Janeiro. We measured the noise level by decibel DEC-460 for five non-consecutive days and nights at five different hours. After a descriptive analysis of data, we performed a study of linear regression.
Results: We identified an average of 62.64 dBA, with a standard deviation of 6.893 dBA and peak of 82.5 dBA during the daytime. The linear regression found that 44% of the variability of the noise is explained by the covariables.
Discussion: The noise levels identified exceed recommendations of national and international organizations. We identified the professional actions and interactions as the main sources of noise.
Conclusion: There is an urgent need to rethink this environment and establish educational strategies for noise reduction, making it safer and healthier.
Descriptors: Noise; Pediatric Nursing, Intensive Care Units, Pediatric.
INTRODUCTION
The pediatric intensive care unit (PICU) is prepared to assist children aged between 29 days and 18 years of age who are in a serious condition requiring immediate and specialized assistance, with the primary objective of saving lives, and returning the child to social conviviality with no, or the least number of possible, sequels. For the success of this assistance, modern monitoring equipment and life support are necessary, as well as a multidisciplinary team(1) responsible for a high number of professionals and numerous stimuli. Though this environment has shown benefits in restoring the health of the child, it also has its negative effects of a physical and psychological nature. This group of factors combined with the complexity inherent in the unit generates stress for patients, families, and professionals, in which case high levels of noise is one of its causes(1,2).
High levels of noise can cause stress, psychological disorders, and sleep disorders. Psychological changes involve behavioral disorders, which are the result of physiological responses to stress that may even interfere with the evaluation of patient sedation(2) The physiological effects begin from 65 dBA, when the hypothalamic-pituitary-adrenal gland is sensitized in adults. In this condition, there are a number of events that can occur, including the secretion of high levels of adrenaline, noradrenaline, and corticosteroids, with consequent elevation of blood pressure, heart rhythm, and peripheral vasoconstriction disorders, as well as interference in the assessment of sedation in critically ill patients(2).
Noise can cause changes in all body systems; it interferes with work, rest, sleep, and communication, in addition to damaging hearing and causing physiological and psychological reactions(3). High noise levels are especially harmful to children, infants, and newborns who are at greater risk of developing stress-related behavioral disorders(3). The psychological effects are linked to the nature of the sound; however, loud noises can affect the child's personality and reduce their capacity for coping with their diseases or traumas(3). In addition, excessive noise has direct interference on sleep, generating insomnia, which is related to immunosuppression, impaired protein synthesis, confusion, irritability, disorientation, lack of control, and anxiety, thus consuming the energy needed for the process of restoration of health(3).
Given the high noise interference in terms of the physical and psychological health of the child, the purpose of this research was to measure the noise levels of the inpatient unit in a Pediatric Intensive Care Sector and to discuss the consequences of environmental noise in terms of professional actions.
METHOD
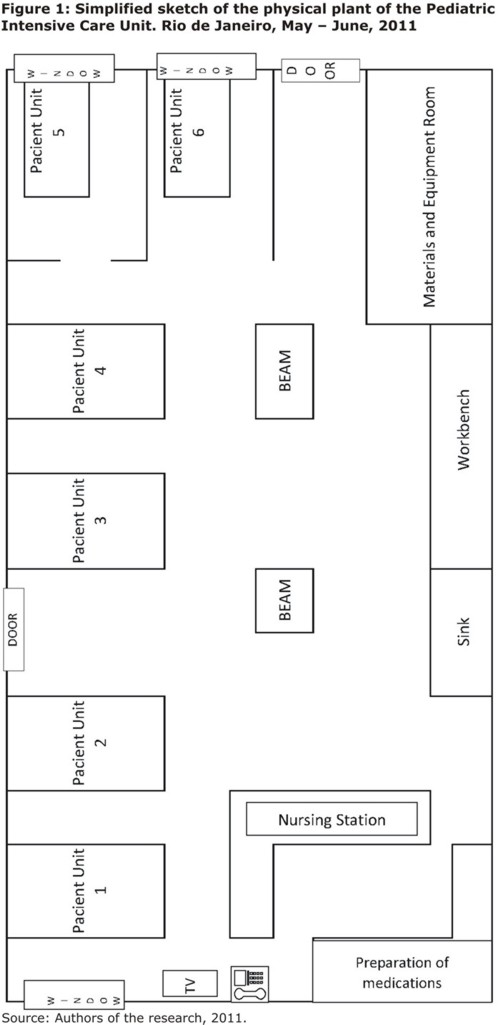
This observational and correlational study was conducted in a six-bed PICU of a federal hospital, which is a benchmark in maternal care and childcare, and this study is aimed towards teaching and research and assistance. Data was obtained between May 19 and June 9, 2011. The unit used to measure the data has an area of 77.17 m2 and presents mixed characteristics, that is, it is composed of four beds in a common area, with washable partitions (curtains) and two beds in a closed area (boxes) with glass panels. Of these boxes, one has no door and on the other, the door would be kept closed only in case of respiratory isolation. The glass panels facilitate the visualization of children and, consequently, increase the capacity of observation and supervision. Also in the hospital, located on a higher and stepped-down area, is the nursing station. It has no central monitoring for preventing equipment alarms to be programmed to a milder sound level.
At PICU the doors have no locks and the floor is rubberized, suitable for a hospital, minimizing noise from the movement of people. The unit is composed of several pieces of equipment necessary for the provision of care of critical patients and use of a multidisciplinary team, which, although important, are sources that produce noise. Among such equipment, there are: computers; telephones; televisions; micro systems; multiparameter monitors; defibrillators; pulse oximetry; capnography; transesophageal monitors; various fans; vacuum absorbers, and; oxygen. Furthermore, the unit features infusion pumps, oxygen transport bullet, litter, scale, gas meter appliances, an X-ray machine, and cleaning equipment such as a washer and floor polisher, in addition to handsets of the professionals working in the sector. The simplified sketch of the physical layout of the unit can be seen in Figure 1.
The multidisciplinary team of the unit is composed of nurses (staff, residents, trainees, and specialization trainees), nursing technicians (staff and trainees), doctors (staff and residents), and a physiotherapist, totaling in the sector, simultaneously, about 20 professionals during a day shift and seven during a night shift. It is worth mentioning the presence of other professionals who are not continually present, such as an occupational therapist, speech therapist, psychologist, radiology technicians and various experts, as well as the presence of relatives and visitors of patients.
To obtain the data and to avoid random errors, the research was performed using the standardization of the measurement method and involved the training of observers (two nurses belonging to the staff of the PICU). The sound pressure levels (SPL) were obtained with a DEC-460 decibel meter model with measurements in weighted decibels (dBA), calibrated and manufactured according to the specifications of the International Electrotechnical Commission (IEC) number 60651. This reference is adopted by NBR 10152(4) of the Brazilian Association of Technical Standards (ABNT, in Portuguese). Because of the inability to position the decibel meter in the center of the rooms and at a distance of 1 m from the ceiling (as recommended by the literature)(4) due to the large influx of professionals and the specific routine of the service and physical arrangement of the area, we opted for individualized assessment in the six beds, that is, in each patient unit. The measurement was performed in a non-concurrent way due to the existence of only one decibel meter. The selection of measurement sites was performed from the physical plant of the unit, obtained by the researchers. The choice of these points aimed at obtaining information that could reflect the level of noise to which the child was being subjected.
Samples were collected for five non-consecutive days in three hours during daytime (8am, 12pm, and 4pm) and in two hours during the night period (11pm and 4am), totaling 150 measures. The hours were predetermined in order to measure sound pressure levels at times of different activities (peak hours for routine activities versus observation time), in order to obtain as much data as possible. Numerical data (dBA), the activities performed by professionals and sources (equipment, actions and interactions of people) that produced noise at the time of collection were recorded in a field diary built by researchers.
For the results to be always achieved in the same place, we established as a measurement point the intersection obtained at a distance of 30 cm from the patient's earlobe and 20 cm from the bed mattress.
The collection period and the sequence with which it was held (non-consecutive days) was defined according to the availability of nurse observers and the little time available, due to previously scheduled work in the unit with an expected duration of one year, which impeded data collection.
After analyzing the data collected, a model for multiple linear regressions was adjusted, having the SPL as a variable response. All significant variables at the 10% level in the univariate model were included in the multivariate model. The variables that remained significant at the 5% level were kept in the final model. The modeling strategy used was the non-automatic "stepwise-backward." The assumption concerning the models of multiple linear regressions (normality and independence of errors and homoscedasticity of variance) were checked by means of residual analysis.
To assess the multicollinearity we used the Variance Inflation Factor (VIF) in which values VIF>10 were considered multicollinear(5). As a result of the adjustment of the regression model we presented estimates, the standard error that measures the uncertainty of these estimates and the p-value that indicates the significance of the covariate. In all analyses, the level of significance of 5% (p-value≤.05) was considered. All analyses and graphics were performed in the program R(5) version 2.15.1.
The research protocol was approved by the Research Ethics Committee of the referred institution, under number 0021.0.008.000-11. It is worth mentioning that this study is part of the ongoing investigation projects of two authors from the Master’s Course in Nursing and the Doctorate in Nursing and Biosciences, both from the Federal University of the State of Rio de Janeiro.
RESULTS
The SPL of the PICU ranged between 44.1 dBA and 82.5 dBA, including day and night periods, with an average of 62.64 dBA and standard deviation of 6.893 dBA. The noise peak occurred at 4pm, in the unit of patient 1 (located next to the nursing station), with 82.5 dBA measured during the presence of four professionals who provided assistance. This bed, whose measurement was performed at 11pm, was also the one that presented the second highest SPL (78.8 dBA). In an extra measurement, during the admission of a child in a gastric transposition postoperative condition, the value of 79 dBA was obtained, due to communication between professionals, furniture being dragged, and equipments alarming. This value was not part of the statistical analysis because it was measured at that time only for comparison with other values.
The highest noise levels were observed in the units of patients 1, 2, 3, and 4, which are closest to the nursing station used by almost all of the multidisciplinary team, not only by the nursing staff. The nursing station is used for the preparation of medications and houses the notes of medical and nursing staff (and other professionals when necessary). It is also the place where the television and phone of the PICU is located. Graphic 1 shows the box-plot of the sound pressure level found for each patient unit.
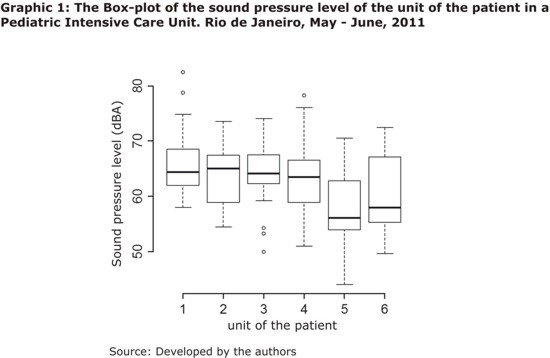
Graphic 1 shows that patient units 5 and 6, used as insulation boxes, had the greatest value variation and the lowest median. These are the most physically distant boxes from the nursing station and accommodate, in most cases, the patients with lower clinical complexity due to little space. This fact generates some difficulty for the use of many types of equipment in tandem with the presence of the multidisciplinary team that needs to get around the units to provide assistance. With the reduction of the patient's clinical complexity and the amount of equipment used in such patient units, it is found that the number of procedures and actions performed by the multidisciplinary team is lower than in other patient units. With this, there is also a reduction in the median of SPL of these units compared to others, which raises reflection on the influence of noise coming from the professionals during daily care activities. Yet the previously mentioned units are influenced by external noise since both have windows, which, although they remain closed, allow the entry of noise from the corridor of the hospital to the patient's unit.
Another extreme value that caught our attention on unit 1 (78.8 dBA) occurred at 11pm: while the cleaning staff were using the floor polisher and conducting conversations loudly.Likewise, in unit 3, we identified a high value (78.3 dBA,) during the crying of an infant hospitalized in the unit, whose sounds were being measured.
In Graphic 2, we found that the SPL varied the time of collection, presenting higher or lower levels, which is believed to be related to the number of professionals at the PICU at the different times considered.
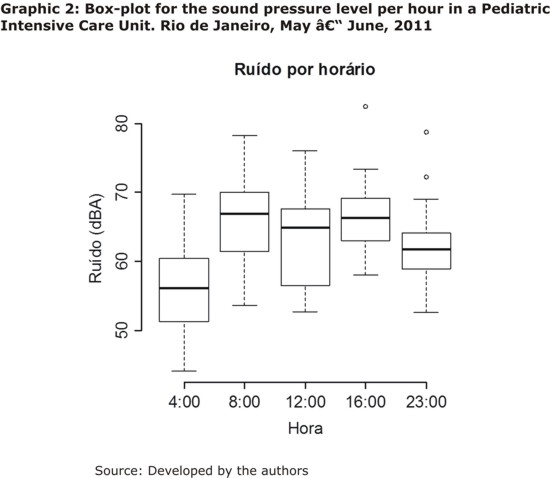
It can be verified in Graphic 2 that the schedules that have the highest noise values are those between 8am and 4pm, which are the times when there are no pre-established routines in the sector in which professionals may or may not conduct some kind of activity in units containing patients. However, the medians remain above 60 dBA, demonstrating that the PICU, as a physical space, has a high noise level, easing up only during late night hours (4am), which showed an average of 56.12 dBA.
Based on the characteristics of the unit and the existence of variables, in which there may be some interference in the production of noise, researchers produced a grouping that has enumerated, among others, a variable called “professionals.” This variable was composed of the activities shown in Table 1.
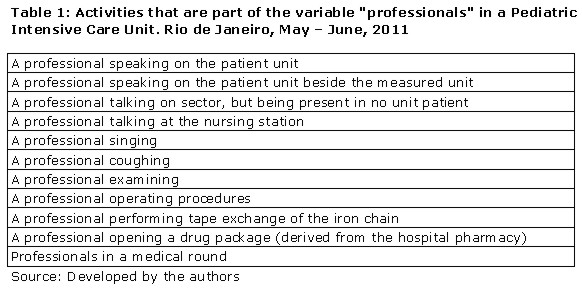
The variable "professionals" showed a clear distinction in the noise values, as seen in Graphic 3. The graphic was represented by the presence or absence of events related to the variable "professionals."
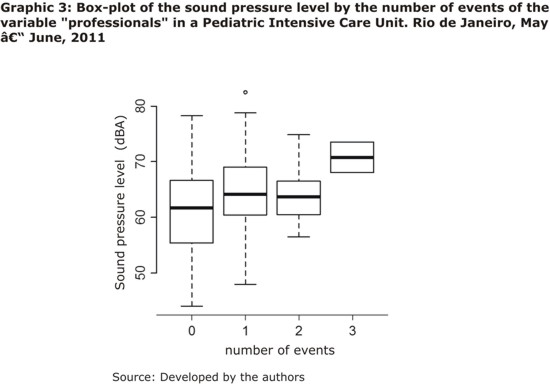
Using Graphic 3, we noted a relationship between the increase in the number of events related to professionals and the increase in noise median, exceeding 70 dBA, remaining highly concentrated at high levels. It can still be observed that, even in the absence of events related to this variable, the patient unit reached high sound pressure levels, reaching heights of almost 80 dBA.
The exploratory analysis allowed us to identify that the SPL is influenced by covariates: time, patient unit, and the professional activity (Graphics 1, 2, and 3), while modeling allowed the quantification of such influences.
According to the results of the multiple linear regression model and considering the response variable SPL (dBA) and the schedules as covariates, the unit of the patient and the number of events of the variable "professionals," allows for the conclusion, through the Coefficient Determination (R2 = 0.4368), that about 44% of the variability of the sound pressure level is explained by the covariates.
By visual inspection of the qq-plot of the residues and of the scatter graph between the adjusted values and residues (graphics not shown), it was considered that the assumptions of normality, homoscedasticity, and independence of errors were met. Furthermore, the VIF showed all values smaller than 10, concluding that there is no multicollinearity. Thus, all the assumptions of the multivariate regression model were met. Table 2 shows the results of the linear regression model.
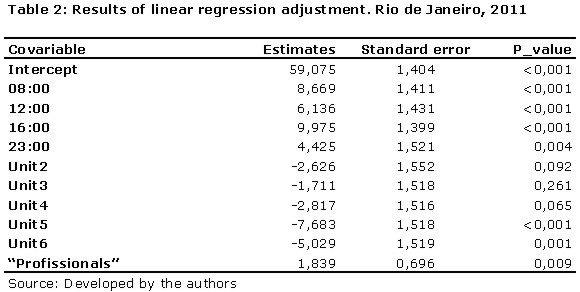
It can be perceived that there is a significant difference among the hours considered, that is, the sound pressure level measured at 4am in the morning is different from the level observed at other times. Furthermore, all the estimates of these parameters (8am, 12pm, 4pm, and 11pm) are positive, meaning that there is an increase in the sound pressure at those times. The p-value of these hours (less than 0.05) indicates that the covariate "hour" significantly influences the response variable (SPL). More specifically, the average sound pressure level is increased by 8.669 dBA when passing from 4am to 8am.
This will be an increase of 6,136 dBA when passing from 4pm to 12pm. It is also evident that there is the influence of the patient unit and it can be concluded that units 2, 3, and 4 are not significantly different from unit 1, but units 5 and 6 are. Moreover, since the estimates of units 5 and 6 are negative, there is a decrease in the sound pressure level if compared to unit 1. As for the number of events of the variable "professionals," there is an influence on the sound pressure level. Furthermore, the increase of a unit of the variable "professionals" leads to an increase of 1,839 dBA in the average sound pressure level, proving to be a major source of noise in the PICU.
DISCUSSION
The Environmental Protection Agency of the United States recommends hospital levels of 45 dBA during the daytime and 35 dBA during nighttime(2). The Brazilian Association of Technical Norms (NBR10152) agrees, suggesting 35 to 45 dBA as acceptable levels for different hospital environments, in which case the first is the desirable level and the second the acceptable limit(4). The American Academy of Pediatrics (AAP) suggests that the amount of ambient noise in pediatric and neonatal ICUs should not exceed 45 dBA(7) and the International Noise Council of the World Health Organization (WHO) recommends a maximum of 40 dBA for internal hospital environments during the day, with a reduction of 5 to 10 dBA for the night period(7). The National Agency for Sanitary Surveillance (ANVISA) does not have regulations for noise in the PICUs. However, the Health Surveillance Secretariat proposes Ordinance 466 of June 4, 1998, not yet in force, which refers to acceptable noise levels according to the recommendation of the International Council of Noise. This council advises that noise should not exceed 45 dBA during the day, 40 dBA in the evening, and 20 dBA at daybreak(8).
The data from the study indicates that the pediatric intensive care unit studied exceeded the maximum levels recommended by official national and international organizations, solely presenting an isolated measure smaller than 45 dBA, which occurred at 4am in the morning. The relationship between the time and the increase or reduction of noise is due to the activities performed and the number of professionals moving around the PICU.
Keeping the focus on the schedule, the data contradicted the expectations of researchers that the PICU’s routine hours (12pm and 11pm) would present higher noise levels due to the amount of activities that have to be performed. However, the data revealed a slight increase in median noise between 8am and 4pm. These hours were intended to provide various types of assistance and there may or may not have been activities in patient units. It is believed that this increase derives from a greater number of conversations, considering the fact that there are no mandatory assistance activities at these hours, leaving practitioners with more time available to relate to others (case discussions and conversations).
During late night hours (4am), a reduction in noise is observed, but not enough to achieve adequate levels, demonstrating that the environment presents itself routinely noisy even without the variable interference from the "professionals." In this case, the noises are probably coming from usual activities like walking by the unit, dealing with objects, and monitoring equipment and life support, connected or alarming.
Data found in a study conducted in a general ICU of a private hospital, which evaluated the stressors for inpatients, identified nurses’ and physicians’ high tones of voice in conversations as one of the stressors(9). This data reinforces the idea that conversations are important sources of noise in the unit, as also identified in this study and demonstrated in Graphic 3. Another study conducted in an ICU of São Paulo, Brazil, found that the greatest noise sources were the health teams and chairs being dragged on the ground, with values of 71.3 and 77.8 dBA, respectively(10).
High noise levels during the night hamper a comfortable rest, causing sleep disturbances, psychological disorders, and even anxiety among most susceptible professionals(9), along with headaches(11), fatigue(11), mood changes(11), and psychiatric disorders(11), as well as influencing professional performance, possibly inducing the professional to distraction(7.9), error(6), and accidents(1).
The ambient noises in hospitals are usually accidental, not chosen, and noise-producers do not have control of volume, duration, location, or cause/effect relations(7). This fact must be known and recognized by the active health team in the PICU in its search for strategies to reduce noise, whether structural, behavioral, or technological. The recognition of noise as a stressor agent for the child and the professional is the beginning of the germination of a healthy and safe environment(12).
The humanization of the PICU environment will involve some consideration of the environmental issues in order to achieve a degree of noise comfort. However, this is still undervalued in the PICU, where the structural planning must combine technology, reception and respect for the patient. The physical structure of the PICU needs to share a favorable workspace for the technical exercise and fulfillment of professionals and patients(7). The recognition of this dual dimension fosters respect for the therapeutic nature of the unit, facilitates the action of the staff, and, above all, does not make it iatrogenic for the patient(13).
An example of environmental imbalance caused by the physical destructuring of the unit can be demonstrated by Graphic 1, where patient units 1 and 2 were the ones that presented the highest median because they were less than 1 m away from the nursing station, the site of greatest professional concentration, beside the telephone and television, while the more distant units showed lower values.
Reinforcing the premise that the physical structure of the PICU contributed to the increase in noise of the patient units closest to the station, meets its limitations in the almost nonexistent publications on the topic of noise in pediatric ICUs, which is a state of affairs that is much more relevant in terms of the neonatal NICUs.
On the other hand, the technology involved in ICU care should also be taken into account as a source of noise, since several studies point to a significant share of the equipment in the production of loud noise.
It is agreed that the construction of healthy spaces includes the control and reduction of ambient noise(14), as well as the awareness of the staff that the health professionals and hospitalized children need to be protected from this adverse environmental hazard, which can irreversibly compromise their health. Several studies on nursing and medical workers’ health claim the need to give greater attention to occupational hazards, among which excessive noise is included(15).
It is necessary, however, to reinforce the concern about the health of children admitted to the PICU concerning the noise, directing our care practices for prevention, with a proactive attitude, rather than focusing our efforts exclusively on the "victims" of this situation(7).
In line with the results found, relating the loud noise to the behavioral character of the multidisciplinary team, it is believed that health education would have a relevant impact on the reduction of ambient noise. Despite the fact that technology contributes to the studied event, it cannot be held responsible for unexpected issues caused to the patient; rather, the human beings who are responsible for its misuse or excessive use are responsible for the misuse of the equipment(16).
The sensitization and reeducation of the health team are fundamental for a change in behavior and an adjustment in behavior is essential in reducing noise(2,11,14). We can suggest a milder tone of voice, conversations with greater proximity between professionals in order to avoid long distance screaming, avoiding conversations beside the patient, and the creation of environments for clinical discussion away from patient units. Moreover, the definition of quiet time, especially at nighttime, with reduced levels of alarm if possible, and volume control of noise-producing equipment (telephones, monitors, life support equipment) are also effective strategies.
We suggest the implementation of a program of continuing education focused on this issue, with the inclusion of the various categories and auxiliary services operating in the PICU. As auxiliary measures, we propose the installation of a continuous sound pressure level measurer, in order to alert the team when levels are exceeded, enabling immediate action, a critical analysis of the physical structure, with discussions aimed at improving the structure focusing on sound comfort and the assessment of the equipments’ noise levels prior to purchase.
CONCLUSION
The PICU studied exceeded the levels recommended by official national and international organizations. It is believed that the implementation of a strategic plan based on behavioral changes can positively impact on the control and reduction of ambient noise, making it safer and healthier for everyone working in the pediatric intensive care scenario. Nursing has a decisive role in this process, as it is represented in a greater number inside the unit and as an important element in the formulation of strategies for improving environmental quality, understanding it as an integral part of the dimension of human care. We reinforce the urgent need for further research in the area of pediatric intensive care.
REFERENCES
1. Sampaio Neto RA, Mesquita FOS, Paiva Junior MDS, Ramos FF, Andrade FMD, Correia Junior MAV. Noise in the intensive care unit: quantification and perception by healthcare professionals. Rev bras ter intensiva [ Internet ]. 2010 Dez [ cited 2012 Aug 15 ] 22(4): 369-74. Available from: http//www.scielo.br/pdf/rbti/v22n4/10.pdf
2. Macedo ISC, Mateus DC, Costa EMGC, Asprino ACL, Lourenço EA. Noise assessment in intensive care units. Braz j otorhinolaryngol [ Internet ]. 2009 Dez [ cited 2012 Aug 15 ] 75(6): 844-6. Available from: http//www.scielo.br/pdf/bjorl/v75n6a12.pdf
3. Aurélio FS. Ruído em unidade de terapia intensiva neonatal [dissertação]. Santa Maria (RS): Centro de Ciências da Saúde da Universidade Federal de Santa Maria; 2009.
4. Associação Brasileira de Normas Técnicas. Níveis de ruído para conforto acústico – procedimento. Rio de Janeiro: Associação Brasileira de Normas Técnicas; 1987.
5. Allison PD. Multiple Regression: a primer. Thousand Oaks: Pine Forge Press; 1999.
6. The R Project for Statistical Computing [ homepage on the internet ]. [ Cited 2012 Aug 03 ]. Available from: http://www.R-project.org.
7. Kakehashi TY, Pinheiro EM, Pizzarro G, Guilherme A. Noise level in neonatal intensive unit. Acta paul enferm [ Internet ]. 2007 Dez [ cited 2012 Aug 21 ] 20(4): 404-9. Disponível em: http//www.scielo.br/pdf/ape/v20n4/02.pdf
8. Ministério da Saúde (Brasil). Secretaria de Vigilância Sanitária. Portaria nº 466, de 04 de junho de 1998. Estabelece o Regulamento Técnico para o Funcionamento dos Serviços de Tratamento Intensivo e sua respectiva classificação de acordo com o grau de complexidade, capacidade de atendimento e grau de risco inerente ao tipo de atendimento prestado. Diário Oficial da União 05 jun 1998.
9. Bitencourt AGV, Neves FBCS, Dantas MP, Albuquerque LC, Melo RMV, Almeida AM, et al. Analysis of stressors for the patient in Intensive Care Unit. Rev bras ter intensiva [ Internet ]. 2007 Mar [ cited 2012 Aug 15 ] 19 (1): 53-9. Available from: http://www.scielo.br/pdf/rbti/v19n1/a07v19n1.pdf
10. Muniz LMN, Stroppa MA. Desconfortos dos pacientes internados na UTI, quanto a poluição sonora. RAHIS. 2009 Jul; 4(3): 56-62.
11. Aurélio FS, Tochetto TM. Noise in a neonatal care unit: measurement and perception of professionals and parents. Rev paul pediatr [ Internet ]. 2010 Jun; 28(2): 162-9. Available from: http://www.scielo.br/pdf/rpp/v28n2/v28n2a06.pdf
12. Miranda EJP, Stancato K. Risks to health of intensive care unit nursing staff: proposal of integral approach of health. Rev bras ter intensiva [ Internet ]. 2008 Mar [ cited 2012 Aug 23 ] 20(1): 68-76. Available from: http://www.scielo.br/pdf/rbti/v20n1/a11v20n1.pdf
13. Silva RR. Psicologia e unidade de terapia intensiva. Revista Salus [ Internet ]. 2007 Jun [ cited 2012 Aug 23 ] 1(1): 39-41. Available from: http:// revistas.unicentro.br/index.php/salus/article/download/668/779
14. Zamberlan-Amorim NE, Fujinaga CI, Hass VJ, Fonseca LMM, Fortuna CM, Scochi CGS. Impact of a participatory program to reduce noise in a neonatal unit. Rev Latinoam enferm [ Internet ]. 2012 Fev [ cited 2012 Aug 17 ] 20(1): 109-16. Available from: http:// www.scielo.br/pdf/rlae/v20n1/pt_15.pdf
15. Fogaça MC, Carvalho WB, Cítero VA, Nogueira-Martins LA. Factors that cause stress for physicians and nurses working in a pediatric and neonatal intensive care unit: bibliographic review. Rev bras ter intensiva [ Internet ]. 2008 Set [ cited 2012 Aug 23 ] 20(3): 261-6. Available from: http:// www.scielo.br/pdf/rbti/v20n3/v20n3a09.pdf
16. Godinho JSL, Tavares CMM. The permanent education in intensive care units: a review article. Online braz j nurs [ Internet ]. 2009 Jun [ cited 2012 Aug 15 ] 8(2). Available from: http:// http://www.objnursing.uff.br/index.php/nursing/article/view/2288
Received: 10/09/2012
Revised: 06/05/2013
Approved: 27/05/2013