ORIGINAL ARTICLES
Early and late pregnant adolescents and neonatal results: a cohort study
Cláudia Carolina Costa1, Ana Paula Pinho Carvalheira2, Caroline de Barros Gomes2, Marli Teresinha Cassamassimo Duarte2, Maria Helena Borgato2, Cristina Maria Garcia de Lima Parada2
1Clinical Hospital of the School of Medicine of Botucatu
2São Paulo State University Julio de Mesquita Filho
ABSTRACT
Aim: To identify the profile of precocious (under 16 years of age) and late pregnant adolescents (17-19 years) by comparing neonatal results.
Method: This is a unique cohort in which potential confounders of a biological and socio-demographic nature were identified (p<0.05), with subsequent analysis of adverse neonatal results in both studied groups, using the chi-square test.
Results: We identified differences in the workplace, first pregnancy, income, labor in the Unified Health System, and cohabitation with a partner. Low Apgar scores and respiratory disorders were more frequent in early adolescents. The need for resuscitation and admission to an intensive care unit did not differ between groups.
Discussion: The studied adolescents revealed that they live in social risk. A relationship was found between Apgar scores and respiratory disorders in the fetuses of early adolescents.
Conclusion: We suggest the need for investment to prevent pregnancy in this age group, and for prenatal care and skilled birth support, especially for precocious adolescents.
Descriptors: Pregnancy in Adolescence; Newborn; Apgar Score.
INTRODUCTION
Teenage pregnancy can be considered a public health problem in Brazil. It can be an unplanned and unwanted event for the teenager herself, her partner and family(1).
Worldwide, it is estimated that 11% of total deliveries of live births are to adolescent mothers, of which 95% occur in developing countries(2).
Data from the Unified Health System (UHS) show that, in Brazil, 20% of all births occurred in this population in 2010, with the majority are mothers being between 15 and 19 years of age(3).
As the adolescents are considered neither children nor adults, pregnancy at this age results in disadvantages related to social, economic, psychological and educational factors, characterizing it as a complex phenomenon(4). In addition to these aspects, studies show that pregnancy during adolescence implies a greater proportion of adverse perinatal results(5), involving such common complications as intrauterine growth restriction(6), low birthweight (LBW)(7), prematurity(7, 8) and low Apgar scores at the fifth minute of life(7).
Scholars agree that maternal age alone is not the only factor and that the perinatal complications of these mothers are bly linked to the dynamics of emotional, psychological, social and economic relationships(9). For them, the risks are linked to multifactorial aspects related to emotional distress, malnutrition, non-compliance or late compliance with prenatal care(10), educational level(9), use of legal or illegal drugs(9) and marital status(5).
Researchers still divide adolescence into early and late, but there is controversy regarding the age limit in the classification of these groups (11). Some studies classify early adolescence when it occurs between 10 and 14 years of age (11), others classify as precocious, teenagers between 10 and 15 years of age (12), and still others, between 10 and 16 years (13).
In terms of adverse perinatal results, both groups depend on factors other than age, such as socioeconomic status and prenatal care (11).
Considering the high prevalence of teenage pregnancies observed in the country, and the possibility of adverse perinatal and neonatal results described in the literature, this study aims to identify the profile of early and late adolescent pregnant women, and compare the adverse neonatal results deriving from these pregnancies, with the intention of contributing to health policies aimed at this population group.
METHOD
This is a study of a historic and unique cohort consisting of a non-probability sample selection calculated in terms of the total births of pregnant adolescents residing in the municipalities that make up the Collegiate "Pole Cuesta Botucatu," that occurred in 2010, as obtained by Datasus (14). The selected women were classified by exposure to pregnancy in early adolescence or in late adolescence. The participants in the research were pregnant women with a single fetus, hospitalized for childbirth care in the period from January 1 to June 30, 2012 in the two maternity hospitals in Botucatu, in the state of São Paulo: one hospital is linked to a public university and the other is characterized as a philanthropic hospital. The first attends parturient women of the Unified Health System (UHS), and is also a reference hospital for obstetric and neonatal high risk cases for the Regional Management Collegiate of Pole Cuesta, which comprises the 13 municipalities of micro-Botucatu. The philanthropic maternity hospital is responsible for private care and supplementary health.
We used secondary data from a larger project that evaluated care during pregnancy, childbirth and puerperium in Botucatu, entitled "The mother-child dyad in Botucatu: an epidemiological study with an emphasis on maternal and infant morbidity and mortality." In this, data were collected from a semi-structured set of open and closed questions. Information was obtained from the medical records of mothers and newborn babies, prenatal cards, nursery rooms and birthing books, and by interviewing the mothers, while still in hospital for childbirth.
The study variables were divided into exposure, potential confounding factors, and outcomes.
It was considered variable from exposure to adolescence in which there was pregnancy (Early/Late). The limit for early adolescence was that the individual had attained 16 years of age, while for late adolescence, the individual had to be between 17 and 19 years of age.
As potential confounders we included the following variables: schooling appropriate to the age in childbirth (Yes/No)(15), work (Yes/No), living with husband or partner (Yes/No), income per capita (R$; median value, minimum and maximum), first pregnancy (Yes/No), alcohol consumption during pregnancy (Yes/No), use of illegal drugs during pregnancy (Yes/No), smoking during pregnancy (Yes/No), planned pregnancy (Yes/No), prenatal care in the UHS (Yes/No), realization of seven or more prenatal visits (Yes/No), participation in educational group for pregnant women (Yes/No), having received information about warning signs in late pregnancy (Yes/No), prescription of folic acid and sulfate ferrous (Yes/No), occurrence of emotional problems during pregnancy (Yes/No), anemia (Yes/No), hypertensive disorders - high blood pressure, pre-eclampsia, eclampsia or HELLP syndrome (Yes/No), diabetes (Yes/No), hemorrhage, bleeding or miscarriage (Yes/No) and infection - syphilis, urinary tract infection, toxoplasmosis, hepatitis, HIV or other (Yes/No), delivery held at UHS (Yes/No), presence of a companion during childbirth (Yes/No), cesarean delivery (Yes/No) and preterm delivery (Yes/No).
The analyzed outcomes were related to the birth condition of the newborn: need for resuscitation of the newborn (Yes/No), Apgar scores on the 1st and 5th minutes ≤ seven points (Yes/No), diagnosis of respiratory disorders (Yes/No), and need for forwarding to the neonatal Intensive Care Unit (ICU) (Yes/No).
Statistical analysis was performed in three steps. The first two were identified by confounding variables, and the third made it possible to relate the age group with the outcomes, correcting the effect of these variables.
In the first stage, potential confounders were identified from the comparison between the age groups in which pregnancy occurred (up to 16 years versus 17 to 19 full years) by means of nonparametric tests: chi-square or The Fisher Exact Test (categorical variables) and by means of the Mann-Whitney Test (numerical variables). The variables that reached p≤0.05 were included in regression models, and were related to outcomes (second stage) in order to confirm them, or not, as confounders.
In the third stage, the relationship between age and outcomes was analyzed by point and interval estimation, with a confidence coefficient of 95% of the Odds Ratios, obtained in models of multiple logistic regressions.
This study was approved by the Ethics Committee in Research, School of Medicine of Botucatu, according to Protocol 4075-2011 and met all the precepts of research involving human beings.
RESULTS
The number of potentially eligible adolescents was 341, of whom 220 were included in the study. Three were excluded because of pregnancies involving twins. Of the total of effectively analyzed adolescents, 33% were early teens. The minimum age was 13 years and the maximum, according to the criterion adopted, was 19.
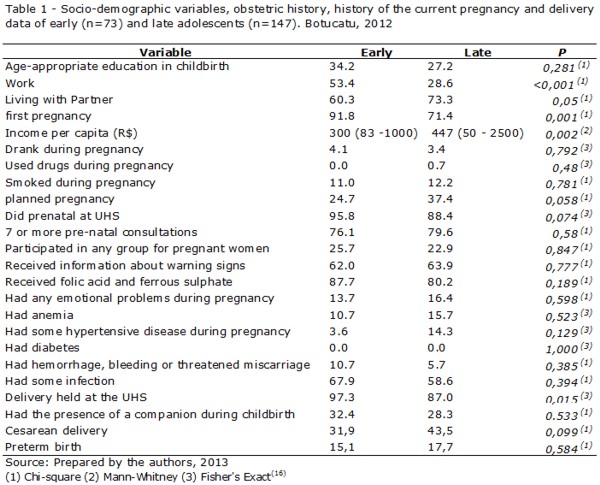
Table 1 shows the socio-demographic profile, obstetric and current pregnancy history and data regarding the delivery of early and late pregnant adolescents, as well as the comparison between the two groups.
In both groups we identified statistically significant differences (p<0.05) when we considered " work status", "first pregnancy", "per capita income" and "delivery in the UHS." The variable "living with partner" was on the borderline of statistical significance. The majority of early teens worked, had no partner, was primiparous, had lower income status and gave birth in the UHS.
In Table 2 we present the list of potential confounders and outcomes studied.
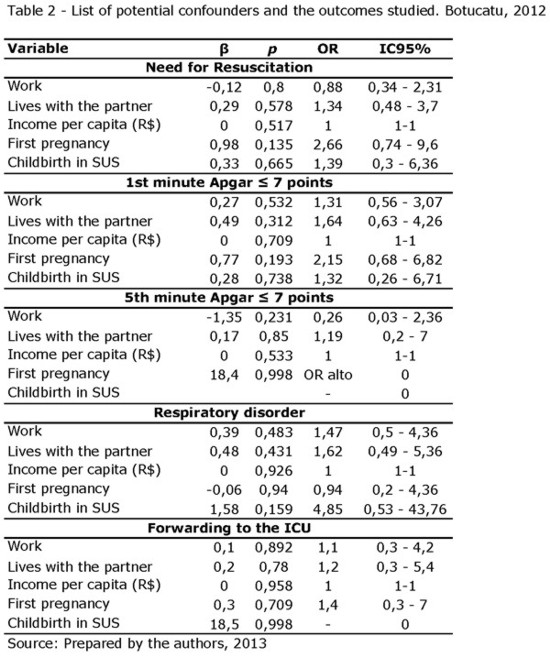
There was no association between potential confounders and the outcomes studied. Therefore, in the investigation of the exposure variable (age of the adolescent) and the outcomes, analyzes adjusted for confounders were not necessary.
In Table 3 we present the prevalence of the outcomes studied, according to the age of the adolescents.
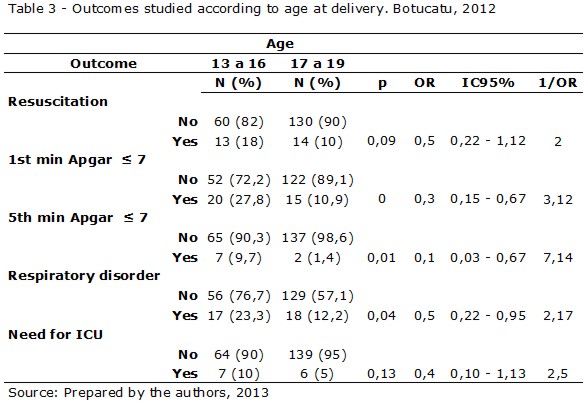
There was no statistically significant difference when considering the percentage of infants receiving resuscitation in the early and late adolescent groups.
We observed a relationship between low Apgar scores in the first minute and the ages of the adolescents (p<0.05). Late adolescence proved to be a protective factor for low Apgar scores, and late adolescents were three times more likely to have scores higher than seven when compared to early adolescents.
The same occurred with the Apgar score at five minutes of life. Late adolescence was also proved to be a protective factor, with a sevenfold higher chance of obtaining scores higher than seven compared with early adolescent mothers.
The diagnosis of respiratory disorders was also significant (p <0.05) when comparing the early to the late group. Mothers between 17 and 19 years of age were twice as likely to give birth to newborns without disorders of the respiratory system compared to adolescents aged 16 years and under.
As for the need for referral to the neonatal ICU after delivery, there was no difference between the groups.
DISCUSSION
This research allowed us to identify the socio-demographic and obstetric profiles of early and late pregnant adolescents treated in a medium-sized municipality of the state of São Paulo from a presumed sample of pregnant women and, thus, the situation found is possibly similar to the situation in other municipalities of the same size.
In the group studied, more than half of the early adolescents worked, differing significantly from the situation of the late teens. These data exceed the proportion of pregnant adolescent women treated in basic health care units in Minas Gerais, as none of the early ones and only 12.5% of the late pregnant women worked (13).
The data found in this study contradicts Brazilian labor law, which prohibits work for children under 16 years of age, allowing us to infer that the adolescents who reported that they were working may be illegally employed, that is, without a formal employment record and, consequently, low paid(13).
Living with a partner also differed between the groups: of the early adolescents, 60.3% lived with a partner compared with 73.3% of the late ones. This means that these numbers are higher than the situation found in the study previously mentioned (13).
Living with a partner may consist of support for these young women, positively impacting on their physical, mental and social state during pregnancy(13), thus, contributing to better outcomes.
The early adolescents had experienced a first pregnancy to a significantly greater extent than the late ones, since 91.8% of them were primiparous, while only 71.4% of the late ones had no other children. This result is in agreement with the literature, which shows a progressive increase in multiparous women with an increase in age(4).
The median per capita income among early adolescents was significantly lower (R$ 300.00) than that of the late teens (R$ 447.00). The variation ranged from R$ 83.00 to R$ 1,000.00 with regard to the younger women and R$ 50.00 to R$ 2.500,00 with regard to the older ones.
According to the Secretary of Strategic Affairs of the Presidency of Brazil, a per capita income between R$ 291.00 and R$ 1,019.00 characterizes the middle class, which means that the lower the level of income, the higher the probability of remaining in poverty (17). Considering the figures cited, it can be stated that some of the studied adolescents are classified as belonging to the Brazilian middle class.
Based on this classification, it can be confirmed that, despite the fact that teenage pregnancy affects the underprivileged social layers, it is also present in a range of different social classes(18).
Based on the results of this study, it can be also stated that if some of these young women do not belong to economically disadvantaged classes, there is an increased chance they may become now, especially when considering that family income will be have to take care of one more individual - the newborn - and also because pregnancy may cause the abandonment of studies, impacting on the future professional life of the mother (19).
Closely linked to income, it is observed that the proportion of births in the UHS was 97.3% among early adolescents and 87.0% on the part of the late ones, indicating a difference between groups.
Although no significant difference between groups of adolescents has been demonstrated, there was great inadequacy as to educational levels: 34.2% of the early adolescents had the appropriate number of years of study for their age, while 27.2% of the late ones were in this situation at the time of delivery. This finding is compatible with other studies that show a relationship between the increased frequency of pregnant adolescents with a reduced number of years of schooling(9,19). The worse situation among late adolescents may be explained by the higher rate of multiparity among them, which may favor the delay or abandonment of studies, due to the pregnancy.
Among the causes of school dropout of adolescents, we may include pregnancy, lack of interest, dislike of studying, laziness and prohibition on the part of the partner(19).
The lower educational level associated with teenage pregnancy brings consequences with regard to economic improvement due to lower qualifications. This increases the chance of these young women working in the informal market and being poorly paid, thus increasing the risk of poverty(18, 20).
The recognition profile of the adolescents allowed the control of an ample amount of confounding factors for adverse perinatal results, involving aspects such as social, economic, emotional and drug use factors, and the occurrence of diseases during pregnancy.
It was observed that the groups of adolescents only differed in terms of income, being employed, living with a partner, being a primiparous woman, and having the baby at the UHS. All these variables were considered to be potential confounders. However, when we investigated the impact of these variables on outcomes, it was found that they are not characterized as such.
The majority of newborns of early adolescents had Apgar scores ≤ 7 both in the first and in the fifth minute, and respiratory disorders at birth. However, there was no difference between the groups studied when assessing the need for neonatal resuscitation and neonatal ICU admission.
Contradicting the results of this study, recent research conducted in São Luis/MA found no association between low Apgar score and maternal age. However, there was an association with the non-performance of prenatal care(11).
In the literature review, we found a close relationship between Apgar scores and respiratory disorders as this score indicates the state of respiratory depression in the newborn in his first few minutes of life(9). Although the low Apgar scores and respiratory disorders among the newborn babies of the early adolescents were more common than in the newborn babies of the late teens, the fact that there was no difference in the need for resuscitation and referral to the neonatal NICU, favors a rapid and positive evolution of these neonates.
A possible explanation for this situation may be related to maternal immaturity at childbirth, resulting in neonatal depression that is quickly resolved. For confirmation, other studies should be conducted to identify the duration of labor of these young women, as well as subjective aspects related to this experience.
CONCLUSION
Neonatal outcomes regarding low Apgar scores were different in the first and fifth minutes and in terms of diagnosis of respiratory disorders, with worse results for the early group.
Thus, we highlight the importance of public policies for comprehensive care that include actions to prevent pregnancy to these specific groups, especially for younger adolescents.
REFERENCES
1. Caminha NO, Freitas LV, Herculano MMS, Damasceno AKC. Pregnancy in adolescence: from planning to the desire to become pregnant – descriptive study. Online braz j nurs[ Internet ]. 2010 [ cited 2013 Jan 20 ] 9(1). Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/2872. doi:http://dx.doi.org/10.5935/1676-4285.20102872
2. MPS Notes. Adolescent Pregnancy. MPS Notes. 2008; 1(1):1-4.
3. Departamento de Informática do SUS[ homepage in the internet ]. DATASUS: informações de saúde 2010 [ cited 2013 feb 22 ]. Available from: http://www2.datasus.gov.br/DATASUS/index.php.
4. Gallo JHS. Gravidez na adolescência: a idade materna, conseqüências e repercussões. Rev bioét. 2011; 19(1):179-95.
5. Sass A, Gravena AAF, Pelloso SM, Marcon SS. Resultados perinatais nos extremos da vida reprodutiva e fatores associados ao baixo peso ao nascer. Rev gaúch enferm. 2011; 32(2): 352-8.
6. Congote-Arango LM, Vélez-García MA, Restrepo-Orrego L, Cubides-Munévar A, Cifuentes-Borrero R. Adolescência como factor de riesgo para complicaciones maternas y perinatales em Cali, Colombia, 2002-2007: estudio de corte transversal. Rev colomb obstet ginecol. 2012; 63(2): 119-26.
7. Maciel SSSV, Maciel WV, Oliveira AGL, Sobral LV, Sobral HV, Carvalho ES, et al. Epidemiologia da gravidez na adolescência no município de Caruaru, PE. Rev AMRIGS. 2012; 56(1):46-50.
8. Martins MG, Santos GHN, Sousa MS, Costa JEFB, Simões VMF. Associação de gravidez na adolescência e prematuridade. Rev bras gineco obstet. 2011; 33(11):354-60.
9. Santos GHN, Martins MG, Sousa MS. Gravidez na adolescência e fatores associados com baixo peso ao nascer. Rev bras gineco obstet. 2008; 30(5):224–31.
10. Debiec KE, Paul KJ, Mitchell CM, Hitti JE. Inadequate prenatal care and risk of preterm delivery among adolescents: a retrospective study over 10 years. Am j obstet gynecol. 2010; 203(2): 122-6.
11. Correia AS. Resultados perinatais na gravidez em adolescentes precoces no município de São Luís- MA. São Luís. Dissertação [ Mestrado em Saúde Materno-Infantil ]- Universidade Federal do Maranhão; 2012.
12. Secundo FF, Marques MMM, Silva ARA, Andrade JM, Guedes MIF. Toxemia gravídica na adolescência. Rev baiana saúde pública. 2009; 33(4): 595-604.
13. Gradim CVC, Ferreira MBL, Moraes MJ. O perfil das grávidas adolescentes em uma Unidade de Saúde da Família de Minas Gerais. Rev de APS. 2010; 13(1): 55-61.
14. Departamento de Informática do SUS [ homepage in the internet ]. DATASUS: informações de saúde 2008 [ cited 2013 feb 22 ]. Available from: http://www2.datasus.gov.br/DATASUS/index.php
15. Ministério da Educação. Ensino fundamental de 9 anos: passo a passo do processo de implantação.2.ed. Brasília: Ministério da Educação; 2009.
16. Bussab WO, Morettin PA. Estatística Básica. 6. ed. São Paulo: Saraiva; 2010.
17. Secretária de Assuntos Estratégicos [ homepage in the internet ]. Perguntas e respostas sobre a definição da classe média [ cited 2013 Feb 22 ]. Available from: Disponível em: http://www.sae.gov.br/site/wp-content/uploads/Perguntas-e-Respostas-sobre-a-Defini%C3%A7%C3%A3o-da-Classe-M%C3%A9dia.pdf.
18. Silva FN, Lima SS, Deluque AL, Ferrari R. Gravidez na adolescência: perfil das gestantes, fatores precursores e riscos associados. Rev Eletrônica Gestão & Saúde. 2012; 3(3): 1166-78.
19. Meincke SMK, Oliveira MRP, Trigueiro DRSG, Carraro TE, Gondim ETC, Collet N. Perfil socioeconômico e demográfico de puérperas adolescentes. Cogitare enferm. 2011; 16(3): 486-91.
20. Faria DGS, Zanetta DMT. Perfil de mães adolescentes de São José do Rio Preto/Brasil e cuidados na assistência pré-natal. Arq ciênc saúde. 2008; 15(1): 17–23.
Received: 28/02/2013
Revised: 29/10/2013
Approved: 11/11/2013