Experiences of women with breast cancer: a research-care
Patrícia Peres de Oliveira1, Aryanne Gabrielle Policarpo1, Liziane
Martins da Silva1, Edilene Aparecida Araújo da Silveira1, Andrea
Bezerra Rodrigues2
1 Federal University of São João del-Rei
2 Federal University of Ceará
ABSTRACT
Aim: to know the experience of women with breast cancer, based on the Theory of Transpersonal Care, and to carry out the educational care of these women, while the meaning expressed by the discourses emerged, mediated by the research-care. Method: this is a qualitative study, with 19 women attended in a support association for people with cancer, carried out from September/2015 to June/2016 in Minas Gerais, Brazil. The interview and the participant observation were used to collect the information; the analysis of the elements was based on the thematic analysis. Results: the analysis resulted in three main categories: favoring beliefs and maintaining faith and hope; impressions about the care received; and the nurse in the process of educational care. A humanized and educational care was carried out, with guidelines and education in health, enabling support to the health-sickness-treatment process of the cared-for. Conclusion: actions based not only on scientific knowledge but on transpersonal care with interaction and exchange between the being-researched and the being-researcher were promoted.
Descriptors: Neoplasms; Nursing; Women's Health.
INTRODUCTION
Malignant neoplasm of the breast is the most incident cancer and the second cause of death worldwide in women(1). In Brazil, estimates for the year 2016 indicate that 57,960 new cases of malignant neoplasm of the female breast will be detected. Despite being considered, in most cases, a cancer with a good prognosis, if it is diagnosed and treated early, malignant neoplasm of the breast is still associated with a high mortality rate in this country(2-3).
The diagnosis of malignant neoplasm of the breast is usually overwhelming in the life of the woman who receives it, either through fear of mutilation and aggressive treatments, fear of dying or multiple losses, as far as social, economic and psychological aspects are concerned, which happens most of the time(4-5). People with breast cancer need emotional support and sometimes just a word of comfort, a hug, a little attention or just an individual who hears them about their fears, doubts or perspective of life, that is, a humanized care(1,3).
At this angle, humanization is a complex process, encompassing differentiated prototypes in the understanding of workers, with their beliefs and values, to change behavior. In relationships and intersubjectivity there is a unique process, not marked by generalizations, since different workers, teams and institutions will have different processes in obtaining humanized care skills(6).
When faced with the environment of health facilities, the worker needs to seek artifice to provide care with empathy and creativity. In this way, it is necessary to understand the sense of care and subjectivity involved in this process, with special attention to the universe of the person with cancer, preservation of their particular world and their welfare needs.
In this context, it was decided to understand the experience of women with malignant neoplasia of the breast, based on the Theory of Transpersonal Care of Jean Watson, in order to enable the care of women with cancer under the educational approach. Educational practices need to be seen as forms not only of humanizing care, but as a solution that promotes women's awareness of their rights, stimulating their participation as subjects of care.
Watson's theory considers nurse-client/patient intersubjectivity, from the concept that there is influence of one individual over the other; it is centered on the humanistic principles of care, contemplating the person in the psychobiological, social, spiritual and cultural dimensions(6-8).
Considering the complexity of the subject and the subjectivity that involves the illness due to a malignant neoplasm of the breast and the humanized care, the question was: how is the experience of women with breast cancer facing the health/illness/care process? What educational care favors the understanding of the disease and the treatment of these women?
In order to answer them, it was necessary to determine the following objectives: to know the experience of women with breast cancer, based on the Theory of Transpersonal Care, and to carry out the educational care for these women, as the meaning expressed by the discourses emerged, mediated by the research-care.
METHOD
This is an exploratory-descriptive and qualitative study that used the research-care methodological framework (RC) and the assumptions of Jean Watson's Theory of Transpersonal Care(6-8).
In the late 1970s, Jean Watson developed the carative factors, which were revised and published in the year 2008(7). The 10 care items (carative factors/caritas processes)(7-8) are described in Figure 1.
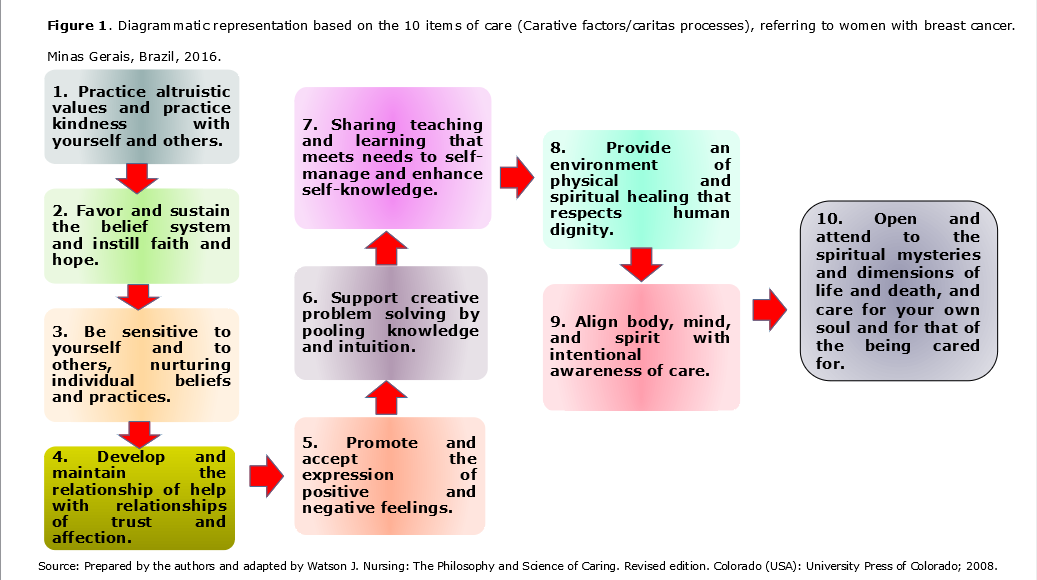
The caritas processes allowed understanding the person in its metaphysical dimension, to direct the concept of healing and to consider the nurse-client intersubjectivity, from the concept that there is influence of one person over the other(6-8).
The RC seeks the connection between care and method, which is not a central focus, but the person searched in its integral essence. It is not only to trigger unveiling and discoveries through method, but rather to illuminate from the perspective of the person's intimacy, focusing on their existence, their possibilities, that is, the essence of experience(9).
To carry out the research-care, one must go through five successive steps: approximation with the study object; encounter of the researcher-caregiver with the researched-cared individual; establishment of research connections, theory and practice of care; removal from the researcher-caregiver individual and researched-cared individual; analysis of the comprehended(9-10).
Approximation with the study object
This approach was accomplished through the development of studies in an association to support people with cancer in a city of Minas Gerais, Brazil, due to their experience as a nurse and researcher.
The choice of the methodological framework served the purpose of the study, since it allowed the development not only of research but also of care actions. In the literature review the subject of the impact of malignant neoplasm of the breast for people with the disease and their family was discussed; nursing care for women with breast cancer; Jean Watson's Theory of Transpersonal Care and the RC from theory to practice. Such discussions helped to approximate the object and to delimit and analyze knowledge with a view to certifying the purposes of the study.
Based on convenience sampling, the following selection criteria were adopted: women older than 18 years of age, breast cancer patients enrolled in an association to support the person with cancer from Minas Gerais, the research scenario, being at any stage of treatment for neoplasia. The exclusion criteria were: women unable to participate in all stages of the RC and inability to understand and/or respond to the proposed issues due to intellectual disability.
Encounter with the being researched-cared for
The initial meeting occurred in an association of support to people with cancer of Minas Gerais or in the domicile of the participant. Firstly, an informal contact was made in order to check availability to be part of the research; later, each interview was scheduled, with a date and time chosen by the participants. The surveyed-caregivers were 19 women with malignant neoplasm of the breast. Nursing care and assistance were carried out in person, based on the needs emerged in each contact, and included activities such as interviews, guidance, clarification of doubts and evaluation.
Perceptions regarding the doubts and needs of the women, as well as nursing behaviors taken were recorded in the field diary and submitted to the thematic analysis. Notes in this journal were used in this article to represent the inferences arising from the data analysis. Prior to the start of the interviews themselves, some identification data were collected from the women: age, treatment protocol, marital status, current occupation, type of residence, and support for treatment.
It is noteworthy that four face-to-face meetings were held with the caregivers. The period of the RC was between September 2015 and June
- The Ethics Committee of the Federal University of São João del-Rei, according to opinion number 1,164,766, was evaluated. The Free and Informed Consent Form was signed, leaving a signed route with the researcher responsible and another with the individuals researched-cared for.
Establishment of research connections, theory and practice of care
This third phase was determinant for the successful application of the RC method, since it relates to the articulation between research (research-care method), theoretical reference (Transpersonal Care Theory) and practice (educational care). In this way, it made possible the approach of the being-researcher-caregiver with the being-researched-cared-for for the interviews. In continuity, the priorities of care were defined, these having been thought in agreement between the participants of the research. Care has been established in different ways: listening, stimulating, guiding, and explaining.
In order to reach the objectives of the study, the listening of the speech was performed without interference from the researcher-caregivers, recorded by a digital recorder. The strategies used in order to achieve the objectives were: the conduct of interviews, according to an instrument prepared by the authors; participant observation while care was performed; and records in the field diary.
The researched-cared-for suggested the preparation of educational manuals, in which the needs of the clients were prioritized, and not only the therapeutic requirements. After the knowledge of this reality and based on the information provided by the researched-cared for, three educational manuals were initially elaborated (care after breast surgery with axillary emptying; care for people taking antineoplastic drugs/chemotherapy for breast cancer; and guidelines for people in radiotherapy for breast cancer), which are in the process of validation as to form and content for later use. It is believed, therefore, that the information will give women greater security for decision-making regarding the procedures required during treatments.
Removal from being a researcher-caregiver and being researched-cared for
This phase required sensitivity of researcher-caregivers and of being researched-cared for in order to deal with the termination of therapeutic encounters. Thus, throughout the methodological trajectory, the women under treatment were prepared for the end of the follow-up.
Analysis of the seized
At this stage, the information from the interviews was transcribed in full. This moment preceded the verification of the elements, which was based on thematic analysis - the form of pattern recognition within the data, in which the themes that emerge are formed into categories(11). In this evaluation, there are multiple forms of approach, such as deductive, based on patterns of predetermined codes known as template, and the inductive, driven by the data. In this study, the chosen method was a hybrid model, that is, it incorporates both the deductive and the inductive(11). In this way, the data are initially analyzed inductively, thus generating codes and initial themes, and then the template is used, in order to identify significant text units, also in a deductive way.
In order to maintain respect for the precepts of ethics in research involving human beings, the researched-caregivers were identified by the term RC, followed by the entry order number of each interviewee.
RESULTS
The 19 surveyed-caregivers were between 42 and 77 years of age, with a mean of 57 years. Most were married, four women declared themselves unmarried, three claimed to be widows and the other three were divorced. As for the occupation, seven women declared themselves retired and the other 12 had formal jobs. All the interviewees lived in urban areas, with access to piped water and basic sanitation, among which 17 lived in their own home and two in ceded residences.
All participants underwent surgery during treatment, with ten women having quadrantectomy and nine undergoing mastectomy of one of the breasts, with removal of the axillary lymph nodes; 15 women underwent adjuvant chemotherapy and radiotherapy and three performed adjuvant radiotherapy alone. Regarding the care received, that is, the use of health services, 15 people exclusively used the services available through the Unified Health System (Sistema Único de Saúde -- SUS), at the three levels of care.
The apprehension about the experience of women with breast cancer was based on the discourse of the respondents-cared for, later divided into three main categories: favoring beliefs and maintaining faith and hope, impressions about the care received, and the nurse in the process of educational care.
Favoring beliefs and maintaining faith and hope
Respect for the other's beliefs, maintaining faith and a physical and spiritual healing environment that respects human dignity are essential elements to maintain the rapprochement between the nurse and the person with malignant neoplasm of the breast and are principles of clinical caritas processes by Watson. Showing women that nursing professionals will always be present, doing their best, demonstrates the importance of ensuring the presence of a committed person at all times, as pointed out in the speeches:
I've had experiences of people with faith. Faith, only faith, healing comes by faith and only God can heal you. There were people who told me, the nurses. (RC12)
They said that those who have faith helped a lot. I'm a Catholic, so I asked God a lot to help the doctors, put God ahead of everything at the time of surgery and also in the treatment... During chemo I said: "Oh my God, don't let me feel bad, don't take me, and bring me without feeling bad". (RC15)
They said that God was in control; with faith everything passes. (RC10)
Prayer and faith are important for recovery. (RC9)
You must have faith... you have to believe that one day it will pass. You have to believe that God protects us; we cannot think that everything is lost. (RC11)
They always talked about God and the importance of faith and I always had faith. I always said, especially because the nurses knew my mother and she had died there, so they always tried to keep me lively and said that every case is a case... put it in the hands of God and have faith that everything would work out. (RC18)
The nurse always gave me a lot of strength... they were always human with me and they were with everyone and always encouraged me when I prayed during the treatment. (RC19)
Impressions about the care received
According to evidence, it was found that the quality of care was evaluated by the women, based on the degree of confidence and affinity with the nurses, care and support during treatment, skills in dealing with people with cancer, support and empathy, and the provision of guidelines on the disease and treatment, as in the following reports:
Sometimes they would help me go to the bathroom, take care of the catheter, and guide me to avoid infection. (RC1)
She was close. She would wait for me to calm down before she put on chemo; she kept talking to me. This was more than creative, it was human. (RC19)
The nurse supported me in everything. (RC13)
Everything comes from the welcome I received from nursing, all thanks to the affection they showed me... I was so well treated, so well cared for that there is no way for me to feel pain. (RC7)
There was much care, with hygiene, with affection, with us, always at disposal. Grade A! Very good! (RC4)
I wanted to die; I didn't want to live... the girls (nurses) went to my house, talked and then it passed. I saw that I won, that I survived. (RC10)
She was always very attentive, so helpful, whenever I needed her, she was there. (RC5)
The nurses were always affectionate with everyone; despite the rush, they always listened when we called. (RC18)
The nurse in the process of educational care
Most caregivers surveyed demonstrated the need for more written information about the disease and therapy through manuals and guidelines. Some did not refer directly to the need for information, but they showed lack of knowledge, as in the following speeches:
She guided me all the time about everything, even on how to proceed inside the bathroom, even in places with lots of people, so I had no problems. (RC14)
The nurse was wonderful; she guided me and cleared my doubts. I asked what I could do after the surgery and she said I could do everything... I am the same person. (RC19)
She was always guiding, always lovingly, with me and with others. (RC3)
In the radiotherapy I was told that I had to go to all sessions, I couldn't miss them. The ink marks on the skin shouldn't be rubbed with soap; the area should be protected from sunlight; I should wear sweaters, comfortable cotton clothes and loose; avoid heat from the stove; avoid contact with people with influenza; I was told this during chemo and radiotherapy. I should always make a light meal; avoid overloading my stomach, but always keeping myself fed. On the left side I can no longer remove cuticles and I cannot let them get this vein. (RC18)
I missed manuals with guidelines; I had doubts at home during the weekends. (RC8)
All that was missing was to deliver in writing all the information. (RC17)
In establishing the true connection with the cared individual, there was a need to provide information to the people under care, so that they could manage their treatment and self-knowledge of their skills. Thus, the lack of use of educational manuals as a strategy for health education, based on scientific evidence, constitutes a gap in care.
Throughout the meetings, the respondents-caretakers participated actively in the elaboration of the three educational manuals previously listed.
DISCUSSION
From the analysis of the results, it can be understood that the care for the woman with malignant neoplasm of the breast was evaluated positively and the researched-cared ones considered the assistance humanized. Reports were collected, in which these women realized that humanization is anchored in care; many authors assert that humanization is not something that occurs automatically and needs to be learned, fostered, and practiced(13-15).
Thus, perceiving the researched-cared women, in the scope of their physical, emotional, spiritual and social needs, demanded from the researcher-caregivers constant reflections and capacities, capable of offering favorable results and creative solutions and with a humanistic approach to problems as components of the caring process(10,14).
The interviewed women's perception about humanized care has brought fundamental elements to human relations, related to Watson's clinical caritas processes(7), such as welcoming, valuing beliefs, instilling faith and hope, communicating, supporting and sharing teaching/learning(8,15), that is, using faith and hope to alleviate the anguish of cancer, since prayer has scientific and spiritual significance(15).In the present study, when reflecting on care from the Transpersonal Care Theory, the caregivers surveyed reported that nurses demonstrated skills in dealing with people with cancer, offering support, empathizing, and giving guidance on the disease and its therapy. The testimonies corroborate the literature, which states that both clients and nurses benefit from a humanized care, since communication is an exchange that brings growth to the life of both(8,14).
Watson's theoretical framework is based on interactivity, assertive communication and intersubjectivity at the moment of care. To that end, nurses need to unite with the person receiving care, in a relationship that perceives the whole(14-15). It is understood that care should not be solely based on scientific knowledge, but also be enveloped by ethical, religious precepts, avoiding empiricism(3,13). In reality, in the elaboration of their care plan, nurses need to explore their own creativity in proposing interventions that aim to facilitate the experience of treatment by women with breast cancer, considering the reality of each one.
The exchange process and empathy are conducive to care: interaction was an important tool for the construction of guidelines manuals and dialogue was essential to establish horizontalized and symmetric interactions between the caregiver researchers and the women participating in the study, since it was based on trust and freedom of expression.
The assistance, through the appreciation of the link, with the recognition of self and of the other, was explained by the participants of this research, which is in line with clinical caritas processes(7) and also promoted a consolidation of the work with the exchange of experiences with women and carers-researchers. Human care involved professional awareness, intentionality, trustworthiness and openness, through the use of the self, outlining the context of the other, seizing the oscillations, senses, sounds, expressions, tones, and forms through which the researched-cared transmitted and reflected their own condition and need(8,13).
Caring in a humanized way is only possible in exchange, in the interpersonal relationship and in the knowledge of the other. Respect for human beings is an essential aspect of humanized care. Meeting the needs of being cared for, believing in their capacity for development and growth are fundamental to a humanized care based on respect for individual needs and faith in the potentialities of being cared for(3). Emotional support, coupled with educational care, besides benefiting the well-being of these clients, stimulated their cooperation and co-responsibility in the care/treatment.
In the reports of the interviewed women, the caregiver-researchers demonstrated respect for the individuality, holistic thinking for the home visiting assistance to the researched-cared for who are more fragile and in despair, extrapolating the rigidity of the routines and functions that permeate the encounter of care, according to one of the elements of the carative factors, which is expressed in helping needs, with intentional awareness of care, administering essential human care(6-8).
It should be pointed out that when approaching women with malignant neoplasm of breast to be cared for, it was appropriate to recognize learning beyond the provision of information, facts or data, but as an exchange, enabling an interpersonal subjective relationship in its essence, which affects the form and context of the process of caring for women.
In this study, most of the surveyed-caregivers reported it was imperative to have greater written information on the disease/treatment. It is believed that education is a moment of the process of humanization, because it is a mediator between the woman with breast cancer and the nurse, in the sense of helping her to achieve the stability lost in the face of the transition of health- disease. This aspect is discussed in the carative factors regarding the importance of sharing teaching and learning in order to meet the needs of the person cared for.
Studies indicate that a printed material can facilitate the understanding of clients, family members, caregivers and other people that relate to women with malignant neoplasm of the breast, since it may contain a greater and more present coverage of the care situation than the resulting one of merely verbal orientations. In addition, it can offer alternatives to many difficulties faced after surgery to treat breast cancer, antineoplastic chemotherapy, radiotherapy, endocrine therapy and biological techniques(16-17). Other research indicates that the lack of knowledge, memory difficulty and vulnerability of the clientele are some of the elements that justify the increase of educational technologies that make dynamic the activities of care (individual or group), which become relevant and essential(17-18), such as client and family orientation manuals.
Educational care is a resource of dual utility: it serves the clients, equipping them for their own care and for the exercise of citizenship, and serves the nurses, for favoring the conquest of space in the professional context. It can be used as a form of interaction between nurses and clients(3-5), since it aims to empower clients for decision, for responsibility, and it happens in the concrete discussion of the reality and the problems experienced by them. The participation of the clients in the educational care is effective through communication, that is, in the exchange between nurses and clients, in the interaction between the parties.
Care, especially educational care, serves as an instrument of transformation as an information exchange in a simple, understandable, true, respectful, but adequate way to the capacity for discernment and understanding of the individuals cared for, facilitating their growth, awareness and exercise of citizenship(8,12-13). Humanism claims that information, decision and responsibility must be shared between the beings cared for and caregivers.
Preparing for self-care and health promotion goes beyond mere information; it is necessary to empower the individuals care for. Therefore, with regard to the task of elaborating interventions for care, the establishment of a process of knowledge is essential for the increase of an educational work with the individuals involved in the search for a better quality of life(16).
In view of this, it is believed that the creation of guidance manuals for people with malignant neoplasm of the breast, after being validated, will advise on the elucidation of women's most recurrent doubts, as well as provide more knowledge for them and their families about all the treatments and favor the understanding of possible complications. All this creates greater security to confront this new phase of the life of women who are experiencing breast cancer and that of their relatives, based on scientific evidence.
In transpersonal care, both the nurse and the person under their care are subject to this bond. They transform themselves and are transformed during follow-up. Thus, the nurse should adopt the use of strategies appropriate to each circumstance(14).
CONCLUSION
This study had positive implications for nursing care, since it enabled the implementation of the theoretical-methodological model proposed by Jean Watson, regarding the follow-up of women with malignant neoplasia of the breast, attached to an innovative approach, RC. In this way, understanding the experiences of women with breast cancer represented a challenge, which was overcome with dedication and effort. We promoted actions based not only on scientific knowledge, but on transpersonal care in a relationship of interaction and exchange between being-researched and being-researcher.
According to the evidence, Jean Watson's transpersonal theory demonstrated affinity with the purpose of the study, showing, besides a nursing theory, a way of being with the other, involving proximity, commitment, empathy and interaction: a continuous search for the autonomy and appreciation of the person.The applicability of the Transpersonal Care Theory allows the nurse working in cancer sectors, whether in the outpatient clinic or in the hospitalization and radiotherapy units, to better understand the experience of women with breast cancer and, at the same time, favor a look at humanistic care. . Thus, as a proposal of humanization to care for the person with breast cancer, nurses can apply the elements of the Clinical Caritas process, which is able to soften the suffering of these women and reduce their apprehensions and doubts.
It is believed that the results of this study can be used by nurses as a support to the planning of care for women with malignant neoplasm of the breast and their family.
The limitation of this study is related to the fact that it was performed with women with breast cancer from a single state of the federation, so that their conclusions portray a specific reality, showing the experience under a given perspective. If performed in other realities, it may elucidate new facets of women with malignant neoplasm of the breast.
REFERENCES
-
Prolla CMD, Silva PS, Netto CBO, Goldim JR, Ashton-Prolla P. Knowledge about breast cancer and hereditary breast cancer among nurses in a public hospital. Rev. Latino-Am. Enfermagem [Internet]. 2015 Feb[cited 2016 Sep 04] ; 23(1): 90-97. Available from: http://www.scielo.br/pdf/rlae/v23n1/0104-1169-rlae-23-01-00090.pdf.
-
Brasil. Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativas 2016: Incidência de Câncer no Brasil [Internet]. Rio de Janeiro: INCA; 2016. [cited 2016 Sept 03]. Available from: http://www.inca.gov.br/estimativa/2016/estimativa-2016-v11.pdf.
-
Oliveira PP, Gesteira ECR, Silveira EAA, AmaralL, Moreira MMC, Rodrigues AB. Evaluation of families with two or more mastectomized women: a case study. Online Braz J Nurs [internet].2016 Mar[cited 2016 Sept 03]; 15(1):83-95.Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/5231/html
-
Barros AG, Melo MCP, Santos VEP. Meanings attributed to cancer by a group of women. Rev enferm UERJ. 2014; 22(1):129-33.
-
Oliveira PP, Maia LN, Resende MS, Macedo RS, Rodrigues AB, Aguiar MIF. Use of the Calgary Family Assessment Model in structural, developmental and functional assessment of the family of mastectomized women with breast cancer. Cogitare Enferm. 2015; 20(4): 661-69
-
Santos MR, Silva L, Misko MD, Poles K, Bousso RS. Unveiling humanized care: nurses' perceptions in pediatric oncology. Text Context Nursing. 2013;22(3): 646-53.
-
Norman V, Rossillo K, Skelton K. Creating Healing Environments Through the Theory of Caring. AORN J. 2016 Nov;104(5):401-09.
-
Olive Ferrer MC, Isla Pera MP. Watson's Model of Caring for a new paradigm in nursing care. Rev Enferm. 2015 Feb;38(2):43-8.
-
Zagonel IPS, Neves EP, Marques KMAP, Iamin SRS, Victor LS. Pesquisa-cuidado da teoria à prática. In: Lacerda MR, Costenaro RGS. Metodologias da pesquisa para enfermagem e saúde da teoria à prática. Porto Alegre (RS): Moriá; 2016. p. 215-50.
-
Ponte KMA, Silva LF, Aragão AEA, Guedes MVC, Zagonel IPS. Clinical nursing care to comfort women with acute myocardial infarction. Text Context Nursing. 2014; 23(1):56-64.
-
Vogt WP, Vogt ER, Gardner DC, Haeffele LM. Selecting the Right Analyses for Your Data: Quantitative, Qualitative, and Mixed Methods. New York: Guilford Publications; 2014
-
Favero L, Pagliuca LMF, Lacerda MR. Transpersonal caring in nursing: an analysis grounded in a conceptual model. Rev Esc Enferm USP [Internet]. 2013[cited 2016 June 12];47(2):500-5. Available from: http://www.scielo.br/pdf/reeusp/v47n2/32.pdf.
-
Borges MS, Santos DS. Caring field: a quantum and transpersonal approach to nursing care. Ciênc Cuid Saúde [Internet]. 2013[cited 2016 June 23];12(3):608-13. Available from: http://www.revenf.bvs.br/pdf/ccs/v12n3/en_26.pdf.
-
González-Hernández OJ. Validez y confiabilidad del instrumento "Percepción de comportamientos de cuidado humanizado de enfermería 3a versión". Aquichan. 2015;15(3): 381-392.
-
Rabelo ACS, Silva LF, Guedes VC, Pon KMA, Silva FVF. Experiences of mothers of children living with cardiopathies: a care research study. Online Braz J Nurs [internet]. 2012 Dec[cited 2016 Sept 03]; 11(3):683-700. Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/3828.
-
Gozzo TO, Lopes RR, Prado MAS, Cruz LAP, Almeida AM. Informações para a elaboração de um manual educativo destinado às mulheres com câncer de mama. Esc. Anna Nery. 2012 June[cited 2016 Sep 05]; 16(2):306-11.
-
Teles LMR, Oliveira AS, Campos FC, Lima TM, Costa CC, Gomes LFS, et al. Development and validating an educational booklet for childbirth companions. Rev Esc Enferm USP. 2014; 48(6):977-84.
-
Áfio ACE, Balbino AC, Alves MDS, Carvalho LV, Santos MCL, Oliveira NR. Análise do conceito de tecnologia educacional em enfermagem aplicada ao paciente. Rev RENE. 2014;15(1):158-65.
All authors participated in the phases of this publication in one or more of the following steps, in according to the recommendations of the International Committee of Medical Journal Editors (ICMJE, 2013): (a) substantial involvement in the planning or preparation of the manuscript or in the collection, analysis or interpretation of data; (b) preparation of the manuscript or conducting critical revision of intellectual content; (c) approval of the version submitted of this manuscript. All authors declare for the appropriate purposes that the responsibilities related to all aspects of the manuscript submitted to OBJN are yours. They ensure that issues related to the accuracy or integrity of any part of the article were properly investigated and resolved. Therefore, they exempt the OBJN of any participation whatsoever in any imbroglios concerning the content under consideration. All authors declare that they have no conflict of interest of financial or personal nature concerning this manuscript which may influence the writing and/or interpretation of the findings. This statement has been digitally signed by all authors as recommended by the ICMJE, whose model is available in http://www.objnursing.uff.br/normas/DUDE_eng_13-06-2013.pdf
Received: 11/08/2016
Revised: 07/03/2018
Approved: 07/03/2018