ORIGINAL
Development of clinical competence by undergraduate students in simulation-based teaching: quasi-experimental study
Ana Cândida Martins Grossi Moreira1, Thaísa Mariela Nascimento de Oliveira2, Maria Gorete Nicolette Pereira2, Caroline Lourenço Almeida Pincerati2, Gisele Andrade Menolli2, Eleine Aparecida Penha Martins2
1State University of Northern Paraná, Bandeirantes, PR, Brazil
2State University of Londrina, Londrina, PR, Brazil
ABSTRACT
Objective: To evaluate simulation-based teaching in the development of students' clinical competence. Method: Quasi-experimental study carried out at a public university with the participation of 62 students. A Knowledge Test and a Checklist were used for data collection. Data were presented as percentages and compared using ANOVA. Results: The average percentage of knowledge, before, during and after the theoretical strategies (case study and dialogued theoretical class), was 67.6%, 76.7% and 88.1% respectively and 87.6% after 30 days. In the simulation, the skill “communicated with clear speech and controlled tone of voice” obtained 93.5% of correct answers; “attached pulse oximeter” and “administered platelet antiaggregant” 100%; 75% of the students classified the patient in one of the three groups of coronary syndrome and 83.7% related it to the best treatment. Conclusion: Simulation-based teaching enabled the development of students' clinical competence in treating coronary syndromes.
Descriptors: Simulation; Clinical Competence; Education.
INTRODUCTION
In recent decades, health education has changed a lot around the world. Active methodologies arise in the context of education, in which the student becomes the protagonist of his/her learning, with autonomy to think about their actions and choices, which favors the development of competencies for care practice(1).
A way of understanding the formation of competences had already been presented in 1990 in Miller's pyramid, which demonstrated that learning for adults went through different levels, from the acquisition of theoretical knowledge to its integration with practice, going through the levels of knowledge, knowing how, showing how and doing(2).
Simulation-Based Teaching (SBT) can contribute to the development of nursing students' clinical competence(3). Simulation is seen as an important active teaching methodology that helps in critical-reflective training and in skill acquisition through integration of theory with practice, identification of errors, recognition of failures and motivation to evolve in the teaching-learning process, which contributes to the decision-making process(4).
In order to obtain clinical competence, which involves knowledge, skill and attitude, simulations can be developed in diverse clinical scenarios such as Acute Coronary Syndrome (ACS). Faced with the current reality of this pathology as one of the main causes of death of the Brazilian population and that the rapid care of patients is essential for better survival(5), it is intended to invest in the training of competent students, future professionals responsible for the care of these patients.
To assess the effect of teaching on students' knowledge, the comparison of knowledge before and after the experience of an educational event can be used. However, it is essential to analyze its retention after a period of time(6), especially in ACS, in which the scientific basis becomes relevant to act quickly and safely, in which every second is important for the patient's prognosis.
The simulation can also contribute to the evaluation of the student's development, which analyzes whether he is able to work safely in his professional life. The skills that need to be improved can be identified during the evaluation of the care simulation, as there is a demonstration of how the actions are carried out, reflecting the mastery of the acquired cognitive, attitudinal and procedural skills(6).
Thus, the objective was to evaluate simulation-based teaching in the development of clinical competence of nursing students for the care of patients with coronary syndrome.
METHOD
This is a quasi-experimental before-and-after study, known as a non-randomized trial or experiment. The research was a single arm, in which all participants were part of the experimental group, developed in the period between February 2019 and February 2020, in which 62 students participated.
The experiment consisted of applying SBT to nursing students at a public university in southern Brazil, in the critical patient module (divided into four groups). The nursing course has been offered by the university for 50 years, and currently has approximately 54 professors and 240 students. Despite the course being organized in an integrated curriculum, in which the professor and the student must be involved in the teaching-learning process in an active and contextualized way, this was the students' first experience with teaching based on simulation. The inclusion criteria in the study was to be enrolled in the fourth year of the nursing course, in the critical patient module, as it is in this period and module that the coronary syndrome class, the subject of the research, is taught. The exclusion criterion was the student having another degree in the health area with competence in caring for patients with ACS, as this could favor their performance in the simulation scenario. The development of the study protocol occurred in three stages and the Model The National League Nursing (NLN) /Jeffries Simulation Theory was used as a methodological theoretical framework(7), which has five components, namely the characteristics of the facilitator; knowledge about the participants; the characteristics of the simulation design; educational practices and the result regarding the skills performed, critical thinking, self-confidence and the contributions of simulation as a teaching-learning method.
The first stage consisted of the construction of a simulation scenario that considered five variables(7), learning objectives, fidelity, problem solving, student support and debriefing, the scenario was also based on a bibliographic review and on the guidelines of the American Heart Association (AHA)(8) on ACS.
A high-fidelity simulation was carried out with an actor patient (student of the nursing residency), in the nursing skills laboratory organized for the service, which aimed to provide assistance to the patient with coronary syndrome by undergraduate nursing students, lasting 40 minutes. Behaviors expected by the participants included, identifying vital signs and intervening, requesting an electrocardiogram, performing a physical examination and anamnesis, administering medication according to the protocol/medical prescription, interpreting an electrocardiogram and classifying the patient into one of the three groups of coronary syndrome. The scenario was validated by the students using the Simulation Design Scale.
In the second stage of the study, the data collection instruments (Knowledge Test and Checklist) were developed by the researchers, based on a bibliographic review through specific books on the subject, scientific articles and the AHA guidelines regarding ACS patient care(8). For the review, the descriptors Patient Simulation, Acute Coronary Syndrome, Clinical Competence and Nursing Students were used, and scientific articles from the last five years were used as inclusion criteria. The Knowledge Test was composed of sociodemographic data and 20 closed theoretical questions, of the true or false type, which aimed to evaluate the students' knowledge regarding ACS. A Checklist for the evaluation of skills and attitudes performed in care simulation, consisting of four indicators and 31 items, developed by the authors and validated through the Delphi technique and expert judges on the subject. Attitudes were demonstrated through assertive decision-making.
In this study, the Checklist indicators were understood as competences to be developed by the students, and the items as technical and non-technical skills, actions to be performed correctly during care simulation. According to the authors, although there are divergences in the literature about the concept of clinical competence, there is a consensus on its elements, composed of knowledge (acquired and accumulated knowledge), skills (knowing how to do specific to the profession) and attitudes (knowing how to act, evaluate and decide(9-10).
SBT implementation occurred during the third stage, and included the application of three teaching strategies, case study, classroom dialogued theoretical class and simulation practice. In the first strategy, the researcher delivered a case study, on the day of the opening of the module, with questions about ACS. The participants were instructed to study and return the questions answered individually, five days later, before starting the previously scheduled dialogued theoretical class.
The theoretical dialogued class lasted 3 hours, using multimedia resources such as Microsoft Power Point, which, associated with the case study, provided a theoretical basis for simulation, according to the objectives of the lesson plan. The students completed the Knowledge Test in four moments, at the opening of the module, after delivering the case study, after the theoretical class and 30 days after the simulation.
The third teaching strategy regarding to care simulation was divided into three phases, as presented below(7). In the pre-briefing and briefing, the students learned about the objectives of the scenario, the physical structure and materials available for use during the activity and asked the students to divide into pairs, lasting 10 minutes. Next, the clinical case was presented to the first pair, randomly chosen, with a request by one of the team members to evaluate a patient with chest pain in the emergency room.
The simulation experience began, simultaneously, with the receipt of the clinical case and the displacement of the pair of nursing students to the emergency room, organized in the nursing skills laboratory, for evaluation and care of the patient actor in 15 minutes. The four observers (evaluators) were positioned behind cardboard screens with glass and one-way film, which allowed the assessment of skills and attitudes, without being viewed by the students. The evaluators were intentionally invited two nursing professors, who work in the fourth year nursing critical patient module, in which the Checklist was applied, and two nursing residents, all with experience in assisting patients with ACS for at least six months.
After the end of the simulation, the facilitator (PhD student in charge of the research) conducted the debriefing with good judgment in pairs, in 15 minutes. All phases were filmed, with the consent of the participants.
Each pair performed the scenario only once, in all, 23 pairs performed the scenario. The time allocated for this practice was 3 days, with an average of eight pairs per day. At each simulation, only the pair, the facilitator and the evaluators remained in the environment, the others were waiting in another room far from the laboratory. After practice, the pair waited in another environment reserved especially for students who had already finished, at the en a general feedback was given to all pairs.
To verify learning retention, the Knowledge Test was reapplied after 30 days, the SBT, as recommended(11).
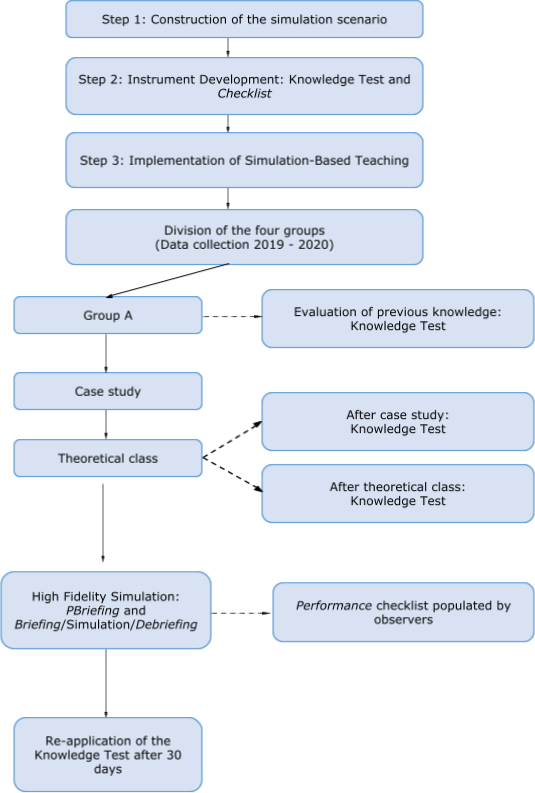
All the steps and activities developed in this study are described in Figura 1:
Source: Prepared by authors, 2019.
Figure 1 - Search flow. Londrina, PR, Brazil, 2019
In care simulation evaluation, the students' skills and attitudes are presented according to the four competencies (communication, patient evaluation, immediate treatment and interpretation of the ECG), which express the performance of the pairs of students and the judgment of four observers. The performance results of 16 students who constituted the first SBT group served as adjustments in the scenario (pre-test for scenario validation) and were not included in the Checklist analysis, thus considering the performance of 46 students, organized in 23 pairs, during care simulation. However, the results of the students' correct answers in the Knowledge Test were counted from the four groups (62 students), because there was no need to change the instrument after the first group.
Regarding data analysis, the information was double-typed in excel spreadsheet and later checked (Exact Formula). Statistical analyses were carried out in the Statistical Package for the Social Sciences® (SPSS) version 20. The categorical data presented in absolute number and percentage, and numerical variables, in mean and standard deviation. The results of the dependent variables were presented with confidence interval (CI) of 95%.
Comparison of the means of the percentage of correct answers, over the four moments in the Knowledge Test, was performed using the ANOVA test for repeated measures. The difference between means, p value < 0.05 was adopted for statistical decision.
This study was approved by the Research Ethics Committee (CEP) in 2018, considering the recommendations of Resolution nº 466/2012 of the National Health Council, with opinion nº 3.093.034, subject to the signature of the Free and Informed Consent Form (TCLE) by the participants.
RESULTS
According to the sociodemographic characterization of the participants, the mean age was 21.44 years (SD±1.49), 57 (91.9%) were women and 5 (8.1%) men, no student had a completed degree course at the time and only one (1.6%) had a technical nursing course.
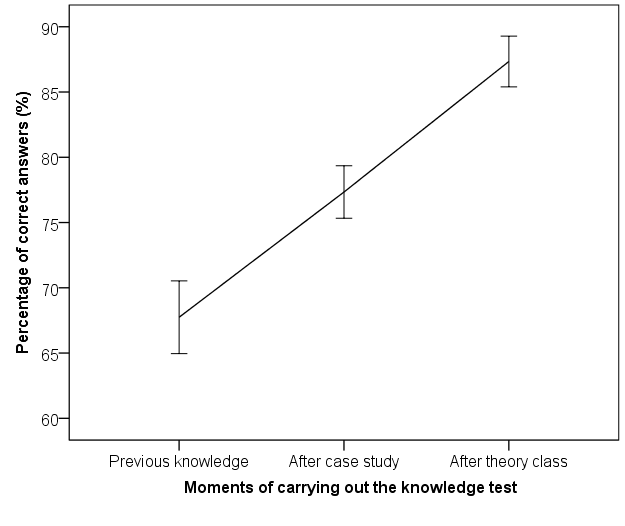
The average percentage of correct answers in the Knowledge Test by the students, over the three moments of the research, is shown in Figure 2.
Source: Prepared by the authors, 2020.
Figure 2 - Comparison of the average percentage of correct answers in the Knowledge Test on care for patients with coronary syndrome, by nursing students (n=62), along the theoretical teaching strategies. Londrina, PR, Brazil, 2019-2020
It is observed that there was a significant increase in the means of correct answers from the first to the second time (Difference 9.0; 95% CI 4.4; 13.6. p < 0.001), and from the second to the third time (Difference 11, 4; 95% CI 8.5; 14.3. p < 0.001).
In Table 1, the data for the competence “communication” are described.
Table 1 - Percentage distribution of adequate performance of non-technical skills during the care simulation for patients with coronary syndrome, for the communication competence. Londrina, PR, Brazil, 2019-2020
Source: Prepared by the authors, 2020.
Legend: * Skill evaluated in 15 pairs observed by 4 evaluators, totaling 60 observations. % = Percentage. CI = Confidence Interval.
Table 2 presents the students' performance in relation to the second competency, "patient assessment".
Table 2 - Percentage distribution of the proper execution of technical skills during the simulation of care for patients with coronary syndrome, for the competence patient assessment. Londrina, PR, Brazil, 2019-2020
|
Competence: Patient assessment |
Proper skill execution |
||
|
Total correct answers recorded by the 4 observers |
% |
CI 95% |
|
|
8. Asked what causes the pain. |
74/92 |
80.4 |
72.3; 88.5 |
|
9. Asked about the quality of pain (burning, tightening, etc.). |
88/92 |
95.7 |
91.5; 99.8 |
|
10. Asked about pain irradiation. |
88/92 |
95.7 |
91.5; 99.8 |
|
11. The pain scale (1 to 10) was used. |
67/92 |
72.8 |
63.7; 81.9 |
|
12. Asked about pain onset time and duration. |
84/92 |
91.3 |
85.5; 97.1 |
|
13. Investigated concomitant symptoms (dyspnea, nausea, etc.). |
23/92 |
25.0 |
16.2; 33.8 |
|
14. Performed ECG in 10 min. |
84/92 |
91.3 |
85.5; 97.1 |
|
92/92 |
100.0 |
- |
|
|
16. Monitored the patient according to equipment specification. |
90/92 |
97.8 |
94.4; 100.0 |
|
17. Verified venous access in the upper limb. |
53/92 |
57.6 |
47.5; 67.7 |
|
18. Placed a contralateral sphygmomanometer for venous access. |
86/92 |
93.5 |
88.4; 98.5 |
|
19. Performed cardiac auscultation in mitral focus. |
47/60* |
78.3 |
67.9; 88.8 |
|
20. Performed pulmonary auscultation at the apex, middle third and base, bilateral. |
44/60* |
73.3 |
62.1; 84.5 |
|
21. Asked about family history on ACS. |
39/92 |
42.4 |
32.3; 52.5 |
|
22. Asked for personal history and risk factors directed to ACS. |
75/92 |
81.5 |
73.6; 89.5 |
|
23. Performed the Fibrinolysis Checklist: |
|
|
|
|
a) Systolic BP > 180 to 200mmHg or diastolic BP > 100 to 110mmHg. |
58/92 |
63.0 |
53.2; 72.9 |
|
27/92 |
29.3 |
20.0; 38.7 |
|
|
c) Asked history of structural disease of the central nervous system (arteriovenous malformation, etc.). |
43/92 |
46.7 |
36.5; 56.9 |
|
d) Asked about significant head/facial trauma in the last 3 months. |
51/92 |
55.4 |
45.3; 65.6 |
|
e) Asked about stroke > 3 hours or < 3 months. |
70/92 |
76.1 |
67.4; 84.8 |
|
f) Asked about major recent trauma (last 2 to 4 weeks) or surgery. |
49/92 |
53.3 |
43.1; 63.5 |
|
g) Asked for a history of bleeding or problems with coagulation or use of anticoagulants. |
70/92 |
76.1 |
67.4; 84.8 |
|
h) Asked about severe systemic disease (cancer, severe liver or kidney disease). |
70/92 |
76.1 |
67.4; 84.8 |
|
24. Requested further tests (cardiac enzymes and chest X-ray). |
65/92 |
70.7 |
61.3; 80.0 |
Source: Prepared by the authors, 2020.
Legend: * Skill evaluated in 15 pairs observed by 4 evaluators, totaling 60 observations. % = Percentage. IC = Confidence Interval.
Some skills in Tables 1 and 2 were evaluated in only 15 pairs of students (indicated with an asterisk), due to the inclusion of these skills in the Checklist from the third simulation group, after the instrument validation process.
The percentages of adequate execution of technical skills in the “immediate treatment” competency are shown in Table 3.
Table 3 - Percentage distribution of the proper execution of technical skills during the simulation of care for patients with coronary syndrome, for immediate treatment competence. Londrina, PR, Brazil, 2019-2020
Source: Prepared by the authors, 2020.
Legend: % = Percentage; CI = Confidence Interval.
Table 4 highlights the performance of students in the competence "ECG interpretation".
Table 4 - Percentage distribution of the proper execution of technical skills during the simulation of care for patients with coronary syndrome, for the competence ECG interpretation. Londrina, PR, Brazil, 2019-2020
Source: Prepared by the authors, 2020.
Legend: Confidence Interval (CI) calculated by the normal approximation method.
According to the evaluation of knowledge retention, after 30 days of SBT, students demonstrated learning maintenance, as the average percentage of correct answers in the Knowledge Test was 87.6%.
DISCUSSION
In the present study, the assessment of students' knowledge revealed a gradual increase after case study (76.7%) and dialogued theoretical class (88.1%), when compared with prior knowledge (67.7%), indicating that the theoretical teaching strategies were effective in apprehending knowledge related to the care of patients with ACS.
Simulation-based teaching as an active learning methodology includes theoretical and practical strategies, which enable learning with situations similar to reality, provides knowledge and skills for a longer time, achieving content fixation in a more motivating way than traditional teaching(12).
With regard to the “communication” competency, students had higher percentages of correct answers related to communication skills with patients during care simulation. However, they did not demonstrate effective communication with the health team, with a low frequency of correct answers in these skills (less than 50%), similarly to leadership and teamwork.
It is inferred that communication and leadership with the team depends on greater professional maturity with greater experience in team coordination. It is expected that these skills are not expressed by many students at this stage of training.
The SBT facilitates the acquisition of non-technical skills such as communication, teamwork and leadership, which are essential from the initial training of future nurses, as it can facilitate the development of a better relationship between patients, family members and professionals, in addition to providing a quality care(13).
The non-technical skills evaluated in the "communication" competency complement the technical or specific skills about ACS that were addressed in the following competencies.
In the competence "patient evaluation", the technical skills with higher percentage of correct answers answered by students are related to cardiopulmonary monitoring (100%), pain assessment (95.7%) and anamnesis (81.5%). On the other hand, the abilities "investigated concomitant symptoms" (25%) and "verified difference of right systolic BP X left > 15mmHg" (29.3%) had a lower frequency of cprrect answers.
A result similar to the percentage of correct answers for the cardiopulmonary monitoring skill was found in a study carried out at the Faculty of Medicine of Ribeirão Preto, in which 83% of candidates for medical residency requested electrocardiographic monitoring during the assessment of clinical competence in the recognition and initial management of Acute Myocardial Infarction with ST Segment Elevation (STEMI) in a simulation station(14).
On the other hand, research carried out at the Beth Israel Deaconess Medical Center pointed out that fourth-year medical students did not adequately perform the patient's anamnesis, demonstrating limited performance in the physical examination during a simulation of chest pain with a high-fidelity mannequin(15).
The “immediate treatment” competency encompasses skills such as oxygen therapy and medication administration according to the protocol(8), in which the students had high percentages of correct answers from 96.7% to 100%, demonstrating decision-making and attitude when performing properly.
It is worth mentioning that, according to the Law of Professional Nursing Practice nº 7.498/86, article 11, item II, paragraph c, the nurse, as a member of the health team, is responsible for prescribing medications established in public health programs and in routine approved by the health institution(17).
As observed in the study with medical participants, 95% administered acetylsalicylic acid and 66% nitrate, in a simulation care station for patients with STEMI(14).
SBT is considered a useful method that provides nursing students with opportunities to exercise skills and decision-making through real experiences without harming the patient's well-being(16).
It is important to remember that, before the administration of medications, students need to make sure that there is no drug allergy, such information was only verified in the simulation by 72.8% of the participants; which demonstrates that this ability needs to be reinforced for safe medication administration, because, considering this as part of the nurse´s role, it obtained a lower rate of percentage of correct answers in relation to the other skills of this competence.
The “ECG interpretation” competency allowed students to develop clinical reasoning and decision-making by identifying leads with ST-segment elevation and relating them to the best form of treatment. The skills of this competency were properly performed with percentages of correct answers that varied from 68.5% to 83.7%. Possessing a quick and agile clinical reasoning, especially in urgency and emergency situations, contributes significantly to the success of professional intervention, to the quality of care provided, which can positively impact the patient's survival(18).
The evaluation of the students' knowledge retention revealed that the acquired learning was significant, with maintenance after 30 days (retention), indicating that the SBT, with different teaching strategies, was effective for obtaining and assimilating knowledge related to the care of patients with ACS. Corroborating this result, a study carried out with medical students, participants demonstrated improvement in knowledge, after intervention through a theoretical strategy with video presentation, and simulated cases on risk stratification of chest pain, and retention evaluated up to five months later(11).
It is possible to verify that educational interventions related to the different teaching strategies, in the patient with acute chest pain, are important in the fixation of the participants' learning(11), as evidenced in the SBT, because, to act in a highly complex simulation scenario, the student needed to be grounded in theoretical knowledge to perform the skills during care, a domain that is not only cognitive but behavioral with decision-making and attitude, articulating different types of knowledge(2) and demonstrating clinical competence, which provides knowledge retention for a longer period of time..
CONCLUSION
The SBT, composed of theoretical and practical strategies, contributed to the development of clinical competence in an ACS scenario. There was a gradual increase in the students' knowledge during the theoretical strategies, case study and dialogued theoretical class, in relation to prior knowledge.
Associated with this learning, the care simulation made it possible to obtain technical skills for patient care with ACS. Non-technical skills were also developed by students, but they showed a lower percentage of adequate performance, with regard to communication between professionals, leadership and teamwork. Participants demonstrated decision-making and attitude when correctly performing the skills.
The pedagogical strategies used were effective and favored knowledge retention of 99.5% by undergraduate nursing students. This study was limited by the fact that the Knowledge Test was not applied immediately after the simulation as to verify the percentage of correct answers by the students.
Thus, this research can collaborate with the political-pedagogical planning of teaching institutions that contemplate active and innovative methodologies such as SBT, particularly in disciplines or modules of urgency and emergency that approach the patient with ACS, for the acquisition of clinical competence in students.
*Paper extracted from the doctoral dissertation “Simulation-based teaching for clinical competence of nursing students in coronary syndrome”, presented to the State University of Londrina (UEL), Londrina, PR, Brazil.
CONFLICT OF INTERESTS
The authors have declared that there is no conflict of interests.
REFERENCES
1. Yamane MT, Machado VK, Osternack KT, Mello RG. Simulação realística como ferramenta de ensino na saúde: uma revisão integrativa. Rev Espaço para a Saúde. 2019;20(1):87-107. https://doi.org/10.22421/15177130-2019v20n1p87
2. Miller GE. The assesment of clinical skills/competence/performance. Acad Med. 1990;65(9):S63-S7. https://doi.org/10.1097/00001888-199009000-00045
3. Bortolato-Major C, Arhur JP, Silva ATM, Mantovani MF, Felix JVC, Boostel R. Contribuições da simulação para estudantes de graduação em enfermagem. Rev Enferm UFPE Online. 2018;12(6):1751-62. https://doi.org/10.5205/1981-8963 v12i6a230633p1751-1762-2018
4. INACSL Standards Committee. INACSL Standards of Best Practice: SimulationSM Simulation-Enhanced Interprofessional Education (SimIPE). Clin Simul Nurs. 2016;12(Suppl.):S34-8. http://dx.doi.org/10.1016/j.ecns.2016.09.011
5. Santos AAA, Braz DDS, Cavalcante AB, Trindade LS, Sá Barros AMM, Souza DS. Identificação precoce da síndrome coronariana aguda: uma revisão bibliográfica. Cad Grad Ciênc Hum Soc Unit (Impr) [Internet]. 2017 [cited 2021 Apr 10];4(2):219-36. Available from: https://periodicos.set.edu.br/cadernobiologicas/article/view/4609/2505
6. Nogueira LS, Wilson AMMM, Karakhanian ACM, Parreira EV, Machado VMP, Mira VL. Avaliação dos conhecimentos e habilidades em ressuscitação cardiopulmonar assimilados por profissionais da atenção primária em saúde. Sci Med (Porto Alegre, Online). 2018;28(1):ID28843. https://doi.org/10.15448/1980-6108.2015.1.19519
7. Jeffries PR. The NLN Jeffries simulation theory. Wolters Kluwer (NY): National League for Nursing; 2016.
8. American Heart Association. Suporte Avançado de Vida Cardiovascular: manual do profissional. Mesquite (TX): Orora Visual; 2016.
9. Unsworth J, Melling A, Porteous D. Developing an integrated approach to the assessment of student nurse competence using the Total Client Care (TCC) assessment tool. Nurse Educ Pract. 2020;44:102757. https://doi.org/10.1016/j.nepr.2020.102757
10.Vreugdenhil J, Spek B. Development and validation of Dutch version of Lasater Clinical Judgment Rubric in hospital practice: An instrument design study. Nurse Educ Today. 2018;62:43-51. https://doi.org/10.1016/j.nedt.2017.12.013
11. Alley WD, Burns C, Hartman ND, Askew K, Mahler SA. 3 for the Price of 1: Teaching Chest Pain Risk Stratification in a Multidisciplinary, Problem-based Learning Workshop. West J Emerg Med. 2018;19(3):613-18. https://doi.org/10.5811/westjem.2017.12.36444
12. Roman C, Ellwanger J, Becker GC, Silveira AD, Machado CLB, Manfroi WC. Metodologias ativas de ensino-aprendizagem no processo de ensino em saúde no Brasil: uma revisão narrativa. Clin Biomed Res. 2017;37(4):349-57. http://dx.doi.org/10.4322/2357-9730.73911
13. Sarabia-Cobo CM, Alconero-Camarero AR, Ibánez-Rementería I. Assessment of a learning intervention in palliative care based on clinical simulations for nursing students. Nurse Educ Today. 2016;26:219-24. https://doi.org/10.1016/j.nedt.2016.08.014
14. Aimoli US, Miranda CH. Clinical Competence in ST-segment Elevation Myocardial Infarction Management by Recently Graduated Physicians Applying for a Medical Residency Program. Arq Bras Cardiol. 2020;114(1):35-44. https://doi.org/10.36660/abc.20180309
15. Bilello LA, Dubosh NM, Lewis JJ, Hall MM, Fisher J, Ullman EA. Fourth-year medical students do not perform a focused physical examination during a case-based simulation scenario. Adv Med Educ Pract. 2018;17(9):583-8. https://doi.org/10.2147/AMEP.S160701
16. Kim SJ, Kim S, Kang K, Oh J, Lee M. Development of a simulation evaluation tool for assessing nursing students’ clinical judgment in caring for children with dehydration. Nurse Educ Today. 2016;37:45-52. http://doi.org/10.1016/j.nedt.2015.11.011
17. Brasil. Lei nº 7498, de 25 de junho de 1986. Dispões sobre a regulamentação do exercício de enfermagem e dá outras providências [Internet]. Diário Oficial da União; 1986 Jun 26 [cited 2021 Aug 28];Seção1:9273-5. Available from: http://www.cofen.gov.br/lei-n-749886-de-25-de-junho-de-1986_4161.html
18. Almeida RG, Mazzo A, Martins JC, Souza-junior VD, Mendes IA. Validation for the Portuguese language of the Educational Practices Questionnaire (Student Version). Acta Paul Enferm. 2016;29(4):390-6. https://doi.org/10.1590/1982-0194201600054
Approved: 01/17/2023
|
AUTHORSHIP CONTRIBUTIONS |
|
Project design: Moreira ACMG Data collection: Moreira ACMG Data analysis and interpretation: Moreira ACMG Writing and/or critical review of the intellectual content: Moreira ACMG, Oliveira TMN, Pereira MGN, Pincerati CLA, Menolli GA, Martins EAP Final approval of the version to be published: Moreira ACMG, Oliveira TMN, Pereira MGN, Pincerati CLA, Menolli GA, Martins EAP Responsibility for the text in ensuring the accuracy and completeness of any part of the paper: Moreira ACMG, Oliveira TMN, Pereira MGN, Pincerati CLA, Menolli GA, Martins EAP |
