ORIGINAL
Content validation of the Hemodialysis Safety Checklist for Brazilian Portuguese: a methodological study
Sara Rebeca de Oliveira Lessa Mendes1, Lais Batista de Lima2, Katarine Lima Moraes3, Clemente Neves de Sousa4, Cecília Maria de Farias Queiroz Frazão1, Vânia Pinheiro Ramos1
1Federal University of Pernambuco, Recife, PE, Brazil
2Hospital of the Clinics of Pernambuco, Recife, PE, Brazil
3University of Brasília, Brasília, DF, Brazil
4Higher School of Nursing of Porto, Porto, Portugal
ABSTRACT
Objective: To perform cross-cultural adaptation and content validation of the Hemodialysis Safety Checklist for use in Brazil. Methods: This methodological study was divided into six stages: i) translation into Portuguese; ii) comparison and synthesis; iii) blind back-translation; iv) comparison and analysis of conceptual, semantic, and content equivalence; v) pilot testing with the target population; and vi) content validation by calculating the Content Validity Index (CVI). Results: The cross-cultural adaptation process resulted in an instrument that was considered precise by the target population after the pilot test. After two rounds of evaluation by experts, the instrument was considered valid, obtaining an Item-Level Content Validity Index (I-CVI) ≥ 0.88 for each item and a Scale-Level Content Validity Index (S-CVI/Ave) = 0.97. Conclusion: The Portuguese version of the Hemodialysis Safety Checklist presents valid content for use in Brazilian hemodialysis.
Descriptors: Patient Safety; Renal Dialysis; Nursing.
INTRODUCTION
Hemodialysis (HD) is a modality of renal replacement therapy for individuals with acute renal failure or end-stage renal disease. Because of the inherent vulnerability of individuals with kidney disease and the specifics of hemodialysis treatment, such as the use of complex technology, invasive procedures, and routine administration of medications that require monitoring, HD is a treatment that is susceptible to the development of activities that pose a risk to patient safety (PS)(1).
PS is a healthcare discipline that aims to study and apply methods to prevent and reduce the risks, errors, and harm that can occur to patients during the provision of care(2). One strategy that has been used in high-complexity settings to promote safer care is the use of checklists(3-5).
Checklists structure care by including a set of behaviors based on the most appropriate care practices according to the literature and professional experience. They are helpful for operationalizing complex routines(6-7).
In 2015, a checklist specifically designed for the context of HD services was developed in Canada, known as the Hemodialysis Safety Checklist. It was constructed using the “Structured Delphi Panel” consensus technique, and its feasibility was tested with frontline nurses in an HD service(3,6).
To develop the items of the Hemodialysis Safety Checklist, the authors conducted a literature review by searching the PubMed database for relevant articles. They also focused on selected resources, such as national guidelines for HD/healthcare quality and the World Health Organization Surgical Safety Checklist(6), to make it a universal language.
The main focus of this checklist is communication between the caregiver and the patient to promote PS. It allows both parties to discuss the treatment plan and correct errors and omissions in care. It also facilitates health education during nursing care(3,6).
The Hemodialysis Safety Checklist consists of 17 items that describe the care to be provided by the nursing team at three different stages of dialysis treatment: i) before the patient arrives at the unit; ii) before HD is started; and iii) after HD is completed. In the study evaluating the feasibility of this checklist, the items related to pre-dialysis weight change, pre-dialysis blood pressure, and intradialytic hypotension showed statistical significance in improving the quality of care(3,6).
For the Hemodialysis Safety Checklist to be used in other countries, such as Brazil, it must undergo a process of translation, cross-cultural adaptation, and validation, which requires careful planning and the adoption of rigorous methodologies. This process ensures greater validity in achieving the objectives proposed by the instrument in different cultures(8).
Therefore, it is assumed that scientific studies that allow the development of tools that can be used to standardize professional practice, based on the theory and professional experience of experts in the field of hemodialysis, facilitate the implementation of the nursing work method, the nursing process, in a safe, evidence-based manner.
To date, no studies have been found that have adapted and validated the Hemodialysis Safety Checklist in other countries through searches of the PubMed and Scopus databases. Therefore, this study aims to develop the process of cross-cultural adaptation and content validation of the Hemodialysis Safety Checklist for use in Brazil.
METHOD
Quantitative methodological research was conducted based on the theoretical framework of Sousa and Rojjanasrirat(8), which includes six stages of development. This framework was chosen because it ranges from the direct translation of the original instrument into the target language (direct or unidirectional translation) to the complete psychometric testing of the final version of the translated instrument in a sample of the target population, thus ensuring the use of the instrument based on scientific evidence.
Stage 1 involved directly translating of the original English instrument into Brazilian Portuguese by two independent translators. These translators were conveniently selected through a specialized translation company. Both translators were bilingual and native speakers of Brazil, with translator 1 being a nurse and translator 2 having a background in English literature. This stage resulted in Target Language Translation versions 1 and 2 (TLT1 and TLT2).
Stage 2 aimed to synthesize the two translations produced in the first stage. To this end, a third bilingual translator (native of Brazil), a nurse and specialist in nephrology, was added to the team. This nurse was selected through a network of researchers in the field. They analyzed the ambiguities and discrepancies in TLT1 and TLT2 and gave their opinion on the best translation for each instrument item. The decisions in this phase were based on consensus between the third translator and the translators from phase 1. This stage resulted in the “Preliminary Initial Target Language” (PITL) version.
Stage 3 was to back-translate the PITL version into the original language using two independent back-translators. Both back-translators were bilingual and native English speakers, with back-translator 4 being a psychologist and back-translator 5 having a background in art. Similar to Stage 1, these back-translators were conveniently selected through a specialized company. This stage resulted in the “Preliminary Initial Target Language” back-translations 1 and 2 (B-PITL1 and B-PITL2).
Stage 4 aimed to compare the discrepancies and ambiguities and determine the semantic, conceptual, and content equivalences in the B-PITL1 and B-PITL2 versions concerning the original instrument. For this purpose, a multidisciplinary committee of six experts was formed: the two translators from the first phase, the two back-translators from the third phase, a methodologist with publications in the field of cross-cultural adaptation of instruments, and a nephrology nurse with experience in hemodialysis. The methodologist was also selected through a specialized company.
The fourth stage was developed through individual assessment of ambiguities and discrepancies and the determination of equivalences for each item of the instrument. A videoconference was then held with all the members of the multidisciplinary committee to discuss the necessary changes to the PITL version to resolve the problems identified and to achieve all the desired equivalences. All decisions were taken by consensus. This phase resulted in the Pre-Final Target Language (PFTL) version.
Stage 5 consisted of a pilot test of the PFTL version with the target population. In this phase, 35 care professionals (assistants, technicians, and nurses) working in the nephrology service for at least six months were conveniently selected. Data collection was done individually by filling out an online form.
The form consisted of questions to assess the clarity of each item using a dichotomous scale that classified each item as “clear” or “unclear”. Data analysis was performed by evaluating the frequency of items considered “clear”, keeping those that received at least 80% of the ratings as “clear”. Frequency calculations were performed using Microsoft Excel 2010.
Stage 6 involved content validation of the instrument by a committee of experts in the construct area of the instrument. This stage included 10 nephrology nurses with one or more characteristics: at least 2 years of experience in the HD unit, publications in nephrology and/or patient safety, or experience in instrument validation. These experts were conveniently selected by analyzing their curricula in the Lattes platform using the keywords “nurse” and “nephrology”.
Data collection was conducted individually by completing an online form. This form consisted of questions to evaluate the clarity (to obtain conceptual equivalence) and relevance (to obtain content equivalence) of each item of the Brazilian version of the Hemodialysis Safety Checklist. The items were scored using a Likert scale with scores ranging from 1 to 4, where 1 corresponded to “not clear/relevant”; 2 to “unable to assess clarity/relevance”; 3 to “clear/relevant but requires minor modifications”; and 4 to “very clear/relevant and concise”.
The data analysis included the evaluation of the degree of agreement between the experts using the content validity index (CVI) per item (I-CVI) and the scale level CVI (S-CVI/Ave). The I-CVI was calculated by considering the number of item ratings of 3 and 4 divided by the total number of rater experts. The S-CVI/Ave was obtained by summing the values of all I-CVIs and dividing them by the total number of items considered in the rating.
An I-CVI greater than 0.80 and an S-CVI/Ave equal to or greater than 0.90 were considered acceptable. Items with different values were re-evaluated, and new CVIs were calculated. To confirm the results, a binomial test was performed to confirm that the proportion of experts rating each item as adequate was not less than 80%. In the statistical analysis of this test, a significance level of 5% was used so that p-values greater than 0.05 indicated that the proportion of experts who considered the item adequate was statistically not less than 80%.
Before conducting the research, permission was obtained from the authors of the original version of the Hemodialysis Safety Checklist to perform its cross-cultural adaptation and validation for use in Brazil. Consent was obtained from participants at all stages of the study by agreeing to the contents of the informed consent form. All procedures followed adhered to ethical principles, and Research Ethics Committee approved the research under opinion number 2.003.629.
RESULTS
The analysis of the versions produced in the first phase revealed differences that, in most cases, did not hinder the understanding of the items but reflected the background knowledge and understanding of the translators. TLA2 was more literal, formal, and faithful to the original version, while TLA1 had a more informal tone, simpler language, and expressions closer to the everyday language used by healthcare professionals.
In the second stage, when analyzing the discrepancies between TLA1 and TLA2 and selecting the best translation for each item to create the PITL version, it was observed that most choices favored TLA1 because its language was closer to the users’ reality. However, some items were adjusted by merging the translations from TLA1 and TLA2 to achieve a more understandable version for the target audience.
In the third stage, the back-translations of the PITL version showed many similarities and deviated from the original version similary. The main influence on the discrepancies between the back-translations and the original version was the choice made in constructing the PITL version, which favored language closer to the context of patient care in hemodialysis in Brazil rather than a more literal translation of the items. The fact that one translator was a health care professional and the second translator had no health care background did not influence a back-translation closer to the original text.
In the fourth step, items that did not meet the three evaluated equivalences (semantic, conceptual, and content) were adjusted in the PITL version. The following changes were made: i) items whose original meaning had been changed in the back translations, with a more literal translation used by the committee; ii) items that contained specific terms related to hemodialysis that confused non-expert translators, so during the committee meeting these terms were clarified with the help of a nephrology specialist participant, and the group identified the best adaptations for the translations; iii) items where words were omitted in the translations, with the necessary corrections made.
In the fifth step, the translated Portuguese version of the Hemodialysis Safety Checklist was pilot-tested for conceptual equivalence (clarity) by 35 individuals from the target population. The average age of these individuals was 36.4 years (minimum: 23 years; maximum: 55 years), the majority were female (94.29%), nurses (62.86%), with a specialization in nephrology (74.29%), and an average of 7.83 years of experience in hemodialysis (minimum: 0.5 years; maximum: 30 years).
During the evaluation of the clarity of the items in the PFTL version of the Hemodialysis Safety Checklist conducted in the pilot test, it was observed that all items received more than 80% of the ratings as “clear” (Table 1), thus meeting the requirements of the translation protocol adopted in this study. Therefore, no changes to the text of the items in the PFTL version were necessary.
Table 1 - Evaluation of conceptual equivalence related to the clarity of the translated Portuguese version of the Hemodialysis Safety Checklist by the target population (n=35). Recife, PE, Brazil, 2021
|
|
Conceptual equivalence |
|||
|
Assessed item |
Clear |
Unclear |
||
|
|
n |
% |
n |
% |
|
Title |
9 |
97,14 |
1 |
2,86 |
|
Phase one title |
32 |
91,43 |
3 |
8,57 |
|
Phase two title |
29 |
82,86 |
6 |
17,14 |
|
Phase three title |
33 |
94,29 |
2 |
5,71 |
|
Item 1 |
35 |
100,00 |
0 |
0,00 |
|
Item 2 |
34 |
97,14 |
1 |
2,86 |
|
Item 3 |
35 |
100,00 |
0 |
0,00 |
|
Item 4 |
35 |
100,00 |
0 |
0,00 |
|
Item 5 |
34 |
97,14 |
1 |
2,86 |
|
Item 6 |
34 |
97,14 |
1 |
2,86 |
|
Item 7 |
35 |
100,00 |
0 |
0,00 |
|
Item 8 |
34 |
97,14 |
1 |
2,86 |
|
Item 9 |
35 |
100,00 |
0 |
0,00 |
|
Item 10 |
35 |
100,00 |
0 |
0,00 |
|
Item 11 |
34 |
97,14 |
1 |
2,86 |
|
Item 12 |
35 |
100,00 |
0 |
0,00 |
|
Item 13 |
35 |
100,00 |
0 |
0,00 |
|
Item 14 |
35 |
100,00 |
0 |
0,00 |
|
Item 15 |
35 |
100,00 |
0 |
0,00 |
|
Item 16 |
35 |
100,00 |
0 |
0,00 |
|
Item 17 |
35 |
100,00 |
0 |
0,00 |
Source: Prepared by the authors, 2021.
For content validation, in the sixth step, the Hemodialysis Safety Checklist was evaluated for conceptual equivalence (clarity) and content equivalence (relevance) by 10 specialists in the field of checklists. The average age of these specialists was 40.9 years (minimum: 28 years; maximum: 56 years), all were female (100%), all were nurses (100%), and all had a specialization in nephrology (100%), with an average of 11.5 years of experience in hemodialysis (minimum: 2 years; maximum: 28 years). Most specialists had a master’s degree with a thesis in nephrology and/or patient safety (60%) and had published articles in this area (80%). Most participants also had experience with content validation (90%). When assessing the content validity of the Brazilian version of the Hemodialysis Safety Checklist, the I-CVI results were satisfactory for most items, with values equal to or greater than 0.90 for the clarity and relevance ratings (Table 2). The S-CVI/Ave obtained was 0.93 for both clarity and relevance.
Table 2 - Content Validity of the Translated Portuguese Version of the Hemodialysis Safety Checklist as Assessed by Experts (n=10) Recife, PE, Brazil, 2023
|
Assessed items |
Conceptual equivalence (Clarity) |
Content equivalence (Relevance) |
||
|
|
I-CVI |
p-value* |
I-CVI |
p-value* |
|
Title |
0,90 |
0,376 |
0,80 |
0,624 |
|
Phase one title |
0,90 |
0,376 |
1,00 |
0,107 |
|
Phase two title |
0,70 |
0,322 |
0,80 |
0,624 |
|
Phase three title |
0,90 |
0,376 |
1,00 |
0,107 |
|
Item 1 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 2 |
0,90 |
0,376 |
0,80 |
0,624 |
|
Item 3 |
0,90 |
0,376 |
0,90 |
0,376 |
|
Item 4 |
1,00 |
0,107 |
0,90 |
0,376 |
|
Item 5 |
0,90 |
0,376 |
1,00 |
0,107 |
|
Item 6 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 7 |
1,00 |
0,107 |
0,90 |
0,376 |
|
Item 8 |
1,00 |
0,107 |
0,90 |
0,376 |
|
Item 9 |
0,90 |
0,376 |
1,00 |
0,107 |
|
Item 10 |
0,80 |
0,624 |
0,80 |
0,624 |
|
Item 11 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 12 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 13 |
0,80 |
0,624 |
0,90 |
0,376 |
|
Item 14 |
1,00 |
0,107 |
0,90 |
0,376 |
|
Item 15 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 16 |
1,00 |
0,107 |
1,00 |
0,107 |
|
Item 17 |
1,00 |
0,107 |
1,00 |
0,107 |
Source: Prepared by the authors, 2021.
*Binomial test
The items that received an I-CVI of less than or equal to 0.8 in the initial evaluation were modified according to the suggestions provided by the experts and then underwent a second round of evaluation. Suggestions from the experts included: i) adding words to the item text to improve comprehension (title, phase 2 title, item 2, and item 10); ii) replacing a literal translation with a new term to clarify the timing of checklist actions (phase 2 title); iii) adding sub-items to one of the items to broaden its scope (item 13). All suggested changes were based on the literature.
In the second round of evaluation, one expert was lost from the sample. In this round, the title, phase 2 title, item 2, item 10, and item 13 of the translated Portuguese version of the Hemodialysis Safety Checklist received an I-CVI equal to or higher than 0.88, resulting in a final S-CVI/Ave of 0.97 for both clarity and relevance (Table 3).
Table 3 - Content validity of the translated Portuguese version of the Hemodialysis Safety Checklist obtained after the second round of expert evaluation (n=9). Recife, PE, Brazil, 2021
|
Assessed items |
Conceptual equivalence (Clarity) |
Content equivalence (Relevance) |
||
|
|
I-CVI |
p-value* |
I-CVI |
p-value* |
|
Title |
1,00 |
0,134 |
1,00 |
0,134 |
|
Phase two title |
1,00 |
0,134 |
1,00 |
0,134 |
|
Item 2 |
0,89 |
0,436 |
0,89 |
0,436 |
|
Item 10 |
1,00 |
0,134 |
1,00 |
0,134 |
|
Item 13 |
1,00 |
0,134 |
1,00 |
0,134 |
Source: Prepared by the authors, 2021.
*Binomial test
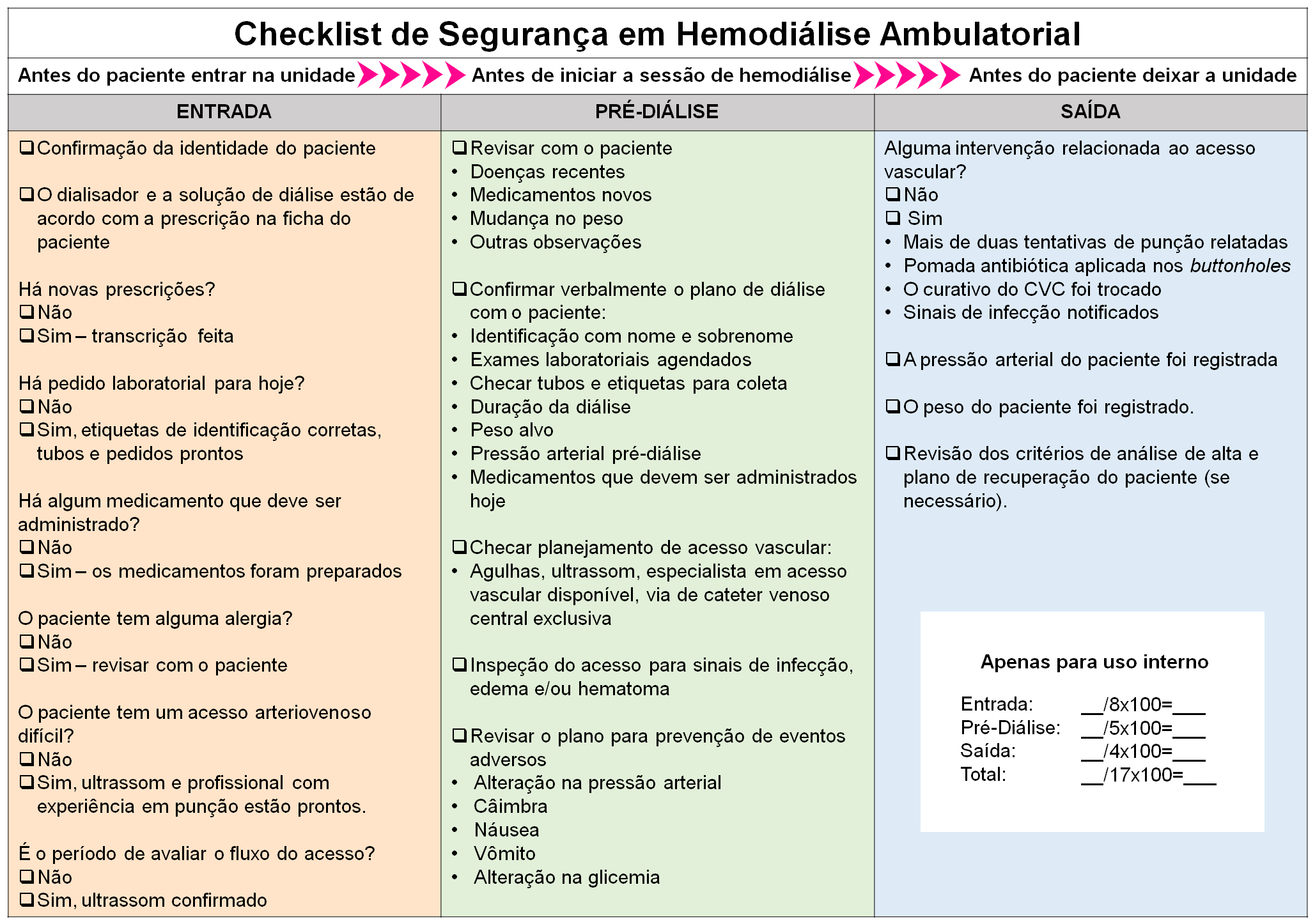
After applying the translation, cross-cultural adaptation, and content validation protocol, the Brazilian version of the Hemodialysis Safety Checklist was named “Checklist de Segurança do Paciente em Hemodiálise Ambulatorial” (Patient Safety Checklist for Outpatient Hemodialysis). This version retained the 17 items of the original instrument; however, due to the need to adapt to the Brazilian context, some items were modified, as can be seen in the final version of the instrument (Figure 1).
Source: Prepared by the authors, 2021.
Figure 1 - Translated, adapted, and content-validated version of the Patient Safety Checklist for Outpatient Hemodialysis for use in Brazil. Recife, PE, Brazil, 2023
DISCUSSION
The Hemodialysis Safety Checklist is a tool that can be used to improve patient safety in hemodialysis and to facilitate health education. It originated in Canada and was made available in English by the authors. Through the process of cross-cultural adaptation and content validation conducted in this study, the tool is now available in Portuguese, validated for the reality of hemodialysis in Brazil, and named “Checklist de Segurança do Paciente em Hemodiálise Ambulatorial” (Patient Safety Checklist for Outpatient Hemodialysis)(3,6).
Regarding the development of the cross-cultural adaptation process, there needs to be a defined protocol in the literature as the best one to use. However, this study shows that the steps of translation, comparison and synthesis, back-translation, comparison and determination of equivalence, pilot testing with the target population, and validation procedures are commonly used by researchers worldwide(9-11).
This information supports the choice of the Sousa and Rojjanasrirat protocol (8) for the development of this work since this protocol includes all the stages mentioned above for the translation and cross-cultural adaptation process of the Patient Safety Checklist for Outpatient Hemodialysis, confirming the reliability of the protocol used.
Concerning the results obtained in the first four stages of the translation and cross-cultural adaptation protocol, the need to adapt some linguistic terms to improve the target population’s understanding was observed, although most items remained faithful to the original version. Cross-cultural adaptation studies often highlight this need in the initial stages, which may involve the exclusion or addition of items to meet the needs of the local reality(12-13).
This aligns with the objectives of these stages, which aim to produce a translated version that is as faithful as possible to the original instrument, considering cultural issues and idiomatic expressions in different languages. Therefore, translation and cross-cultural adaptation procedures should not be limited to reproducing literal word meanings(8).
In this study, similar to a translation and cross-cultural adaptation study conducted in Italy(12), these issues were further discussed in the post-back-translation phase with the participation of experts and the translators involved in the previous phases. In addition, the post-back-translation equivalence evaluation identified some shortcomings in the translation process that could affect the quality of the final translation. These results confirm the importance of a multidisciplinary committee for the evaluation, review, and consolidation of the translation process of instrument items, as well as for a more appropriate cross-cultural adaptation through the evaluation of semantic, conceptual, and content equivalences(8).
Evidence of the quality of translation and cross-cultural adaptation was observed in the results of pilot testing with the target population, as all items were considered precise according to the criteria established by the protocol. The same was observed by the authors of a study conducted in China(14), who considered the success of the translation process of their scale based on the evaluation of the responses of the participants in the target population, who were able to answer the translated questionnaire easily in the vast majority of cases.
Regarding the validation process, this study chose to perform content validation because the Patient Safety Checklist for Outpatient Hemodialysis is a procedural support tool rather than an assessment tool that results in a score. Studies with similar aims to this instrument have also validated their checklists through content validation(13,15-16). The content validation process in this study strengthens the credibility of the result of the translation and cross-cultural adaptation process.
The I-IVC values ranging from 0.88 to 1.00 and the S-IVC/Ave value of 0.97 were obtained after two rounds of expert evaluation. These values are within the standard set by the methodological reference used in this study(8) and are similar to those obtained in studies that also validated the content of their instruments(13, 15-16). During the validation process, some items were adjusted based on the suggestions made by the experts during their evaluation of the instrument.
With regard to its purpose, the Patient Safety Checklist for Outpatient Hemodialysis standardizes the nursing actions that should be followed by the care team during hemodialysis treatment, ensuring that none of the listed procedures, no matter how simple, are overlooked by the healthcare professional(17-18).
In terms of item organization, inspired by the World Health Organization Surgical Safety Checklist(19), the authors of the original instrument grouped the items into three phases of patient care in hemodialysis. These phases highlight strategic pauses that should be implemented during critical moments of care. As a result, they guide care from before the patient arrives at the unit until the patient leaves(3).
In terms of broader patient safety goals, care related to correct patient identification, verification of medical prescriptions for each session, and prevention of infection and/or other vascular access-related complications are consistent with international goals and national patient safety initiatives(20).
The Patient Safety Checklist for Outpatient Hemodialysis may be helpful from a health education perspective. In the second phase of use (“pre-dialysis”), there is a dialogue between the care team and the patient in which the nurse addresses important self-care issues while confirming information with the patient.
CONCLUSION
The Brazilian version of the Hemodialysis Safety Checklist, the Patient Safety Checklist for Outpatient Hemodialysis, showed in the pilot test that more than 80% of the participants rated all items as clear. In addition, it achieved a satisfactory S-IVC/Ave value of 0.97 during content validation.
Therefore, after translation and cross-cultural adaptation, the Patient Safety Checklist for Outpatient Hemodialysis has valid content for use in the reality of hemodialysis in Brazil, intending to promote safety in the care of patients undergoing this treatment. In addition, the tool can also serve as a facilitating tool in health education, creating a space for dialogue between the patient and the caregiver.
Scientific studies that enable the development of tools that can be used to standardize professional practice, such as the Patient Safety Checklist for Outpatient Hemodialysis, contribute to the safe implementation of care processes based on evidence-based practice. This helps to improve the quality of patient care.
*Paper extracted from the master's dissertation “Cross-cultural adaptation and content validation of the “Hemodialysis Safety Checklist” for the Brazilian context”, presented to the Federal University of Pernambuco, Recife, PE, Brazil.
The authors have declared that there is no conflict of interests.
REFERENCES
1. Aguiar LL, Guedes MV, Galindo Neto NM, Melo GA, Almeida PC, Oliveira RM. Validação de instrumento de avaliação da segurança de pacientes renais em hemodiálise. Acta Paul Enferm. 2018;31(6):609-15. DOI: http://dx.doi.org/10.1590/1982-0194201800084
2. World Health Organization (WHO). Patient Safety [Internet]. Geneva: WHO; 2019 [cited 2021 May 02]. Available from: https://www.who.int/news-room/fact-sheets/detail/patient-safety
3. Thomas A, Silver SA, Rathe A, Robinson P, Wald R, Bell CM, et al. Feasibility of a hemodialysis safety checklist for nurses and patients: a quality improvement study. Clin Kidney J. 2016;9(3):335–342. http://dx.doi.org/10.1093/ckj/sfw019
4. Crandell BC, Bates JS, Grgic T. Start using a checklist, PRONTO: Recommendation for a standard review process for chemotherapy orders. J Oncol Pharm Pract. 2018;24(8):609-616. http://dx.doi.org/10.1177/1078155217722594
5. Abbott TEF, Ahmad T, Phull MK, Fowler AJ, Hewson R, Biccard BM, et al. The surgical safety checklist and patient outcomes after surgery: a prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018;120(1):146-155. http://dx.doi.org/10.1016/j.bja.2017.08.002
6. Silver SA, Thomas A, Rathe A, Robinson P, Wald R, Harel Z. Development of a hemodialysis safety checklist using a structured panel process. Can J Kidney Health Dis. 2015;5(2):1-9. http://dx.doi.org/10.1186/s40697-015-0039-8
7. Cardoso ASF, Muller S, Echer IC, Rabelo-Silva ER, Boni FG, Ribeiro AS. Elaboration and validation of a drug administration checklist for patients in research protocols. Rev Gaúcha Enferm. 2019;40(esp):e20180311. https://doi.org/10.1590/1983-1447.2019.20180311
8. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instrumentes or scales for use in cross-cultural health care research: a clear and user friendly guideline. J Eval Clin Pract. 2011;17:268-274. http://dx.doi.org/10.1111/j.1365-2753.2010.01434.x
9. Mansouri A, Motaghedi R, Rashidian A, Ashouri A, Kagrar M, Hajibabaei M, et al. Validity and reliability of the Persian therapy-related symptom checklist. Iran J Med Sci [Internet]. 2017 [cited 2021 May 02];42(3):292-300. Available from: https://www.researchgate.net/publication/317093185_Validity_and_Reliability_Assessment_of_the_Persian_Version_of
_Therapy-Related_Symptom_Checklist
10. Yalin OO, Uludüz D, Sungur MA, Sart H, Özge A. Identification of Allodynic Migraine Patients with the Turkish Version of the Allodynia Symptom Checklist: Reliability and Consistency Study. Noro Psikiyatr Ars. 2017;54:260-266. http://dx.doi.org/10.5152/npa.2016.15953
11. Paiano R, Teixeira MCTV, Cantiere CN, Efstratopoulou MA, Carreiro LRR. Translation and cross-cultural adaptation of the Motor Behavior Checklist (MBC) into Brazilian Portuguese. Trends Psychiatry Psychother. 2019;41(2):167-175. http://dx.doi.org/10.1590/2237-6089-2017-0104
12. CovottaA, Gagliardi M, Berardi A, Maggi G, Pierelli F, Mollica R, et al. Physical Activity Scale for the Elderly: translation, cultural adaptation, and validation of the italian version. Curr Gerontol Geriatr Res. 2018:8294568. http://dx.doi.org/10.1155/2018/8294568
13. Storesund A, Haugen AS, Wæhle HV, Mahesparan R, Boermeester MA, Nortvedt MW, et al. Validation of a Norwegian version of SURgicalPAtient Safety System (SURPASS) in combination with the World Health Organizations’ Surgical Safety Checklist (WHO SSC). BMJ Open Quality. 2019;8(1):e000488. http://dx.doi.org/10.1136/bmjoq-2018-000488
14. Zhou X, Xu X, Fan J, Wang F, Wu S, Zhang Z, et al. Cross-cultural validation of simplified Chinese version of spine functional index. Health Qual Life Outcomes. 2017;15(203):1-9. http://dx.doi.org/10.1186/s12955-017-0785-7
15. Boeckmann LMM, Rodrigues MCS. Adaptação e validação de checklist de segurança cirúrgica na cesárea. Texto Context Enferm. 2018;27(3):e2780017. https://doi.org/10.1590/0104-070720180002780017
16. Batistini HC, Sant’anna ALGG, Giovanazzi RSDG, Freitas VR, Costa SACM, Machado RC. Checklist validation for care provided to patients in the immediate postoperative period of cardiac surgery. J Clin Nurs. 2020;29:4171-4179. https://doi.org/10.1111/jocn.15446
17. Amaya-Arias AC, Zuluaga O, Idárraga D, Eslava-Schmalbach JH. Adaptation and validation for Colombia of the WHO safe childbirth checklist. Colomb Med (Cali). 2018;49(3):201-212. http://dx.doi.org/10.25100/cm.v49i2.2710.
18. Mendes SROL, Pessoa NRC, Santos GMR, Costa NFG, Frazão CMFQ. Strategies to promote patient safety in hemodialysis: An integrative review. Nephrol Nurs J. 2020;47(5),447-454. https://doi.org/10.37526/1526-44X.2020.47.5.447
19. Organização Mundial Da Saúde (OMS). Segundo desafio global para a segurança do paciente: Manual - cirurgias seguras salvam vidas (orientações para cirurgia segura da OMS). Nilo MS, Durán IA, tradutores. Rio de Janeiro: OPAS, Ministério da Saúde, Agência Nacional de Vigilância Sanitária; 2009 [cited 2021 May 02]. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/seguranca_paciente_cirurgias_seguras_guia.pdf
20. Silva RR, Magalhães DCS. A utilização da ferramenta de “Notificação de Ocorrências” como parâmetro avaliativo das metas internacionais de segurança do paciente. Revista Pró UniverSUS [Internet]. 2018 [cited 2021 May 02];09(1):17-24. Available from: http://editora.universidadedevassouras.edu.br/index.php/RPU/article/view/1273
Submission: 05/30/2022
Approved: 07/10/2023
|
Project design: Mendes SROL, Sousa CN, Frazão CMFQ, Ramos VP Data collection: Mendes SROL Data analysis and interpretation: Mendes SROL, Lima LB, Moraes KL, Sousa CN, Frazão CMFQ, Ramos VP Writing and/or critical review of the intellectual content: Mendes SROL, Lima LB, Moraes KL, Sousa CN, Frazão CMFQ, Ramos VP Final approval of the version to be published: Mendes SROL, Lima LB, Moraes KL, Sousa CN, Frazão CMFQ, Ramos VP Responsibility for the text in ensuring the accuracy and completeness of any part of the paper: Mendes SROL, Lima LB, Moraes KL, Sousa CN, Frazão CMFQ, Ramos VP |
